

Biomarkers of sepsis
- PMID: 23480440
- PMCID: PMC3613962
- DOI: 10.3109/10408363.2013.764490
Biomarkers of sepsis
Abstract
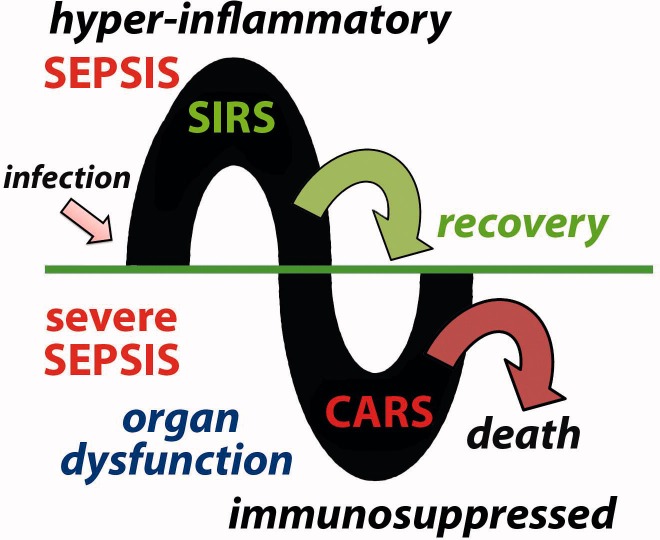
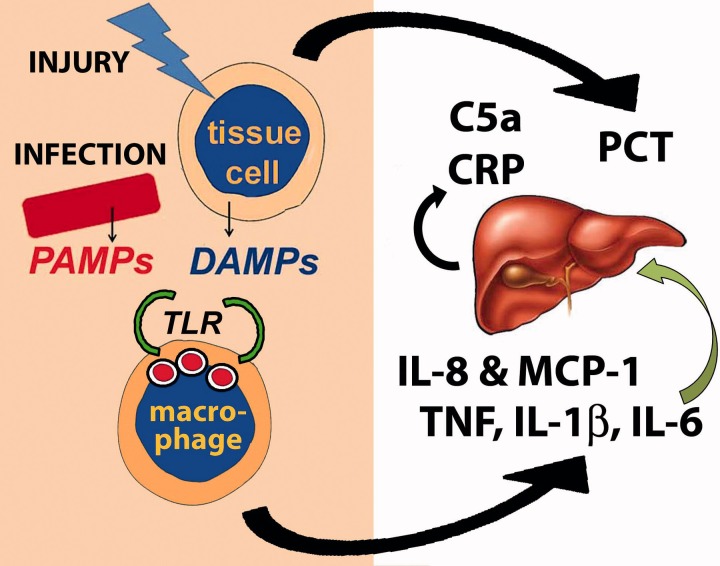
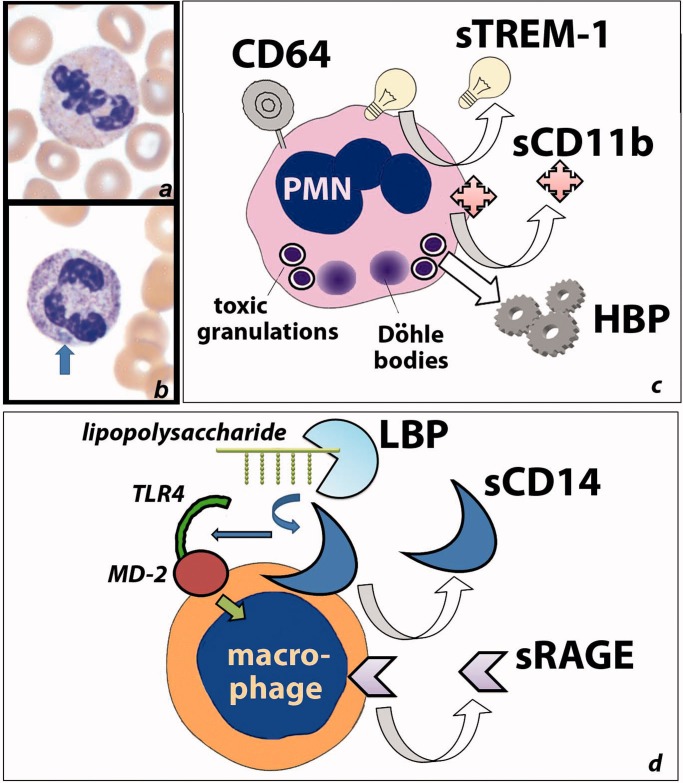
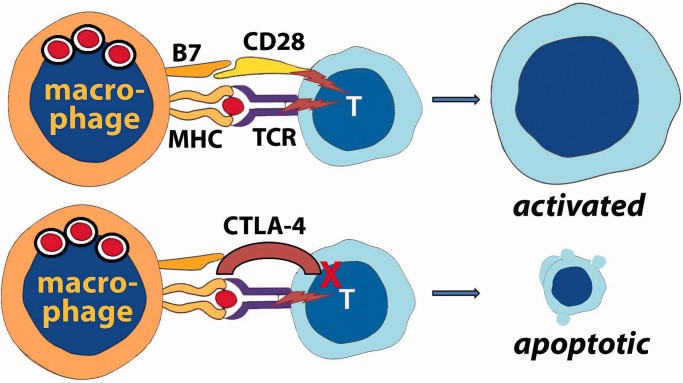
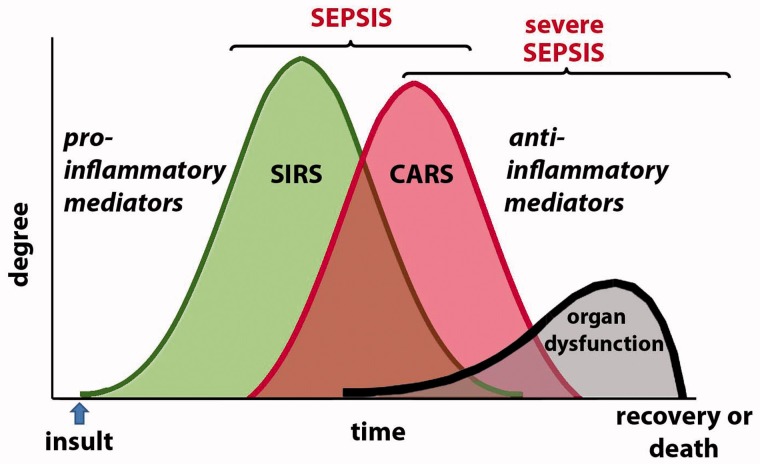
Sepsis is an unusual systemic reaction to what is sometimes an otherwise ordinary infection, and it probably represents a pattern of response by the immune system to injury. A hyper-inflammatory response is followed by an immunosuppressive phase during which multiple organ dysfunction is present and the patient is susceptible to nosocomial infection. Biomarkers to diagnose sepsis may allow early intervention which, although primarily supportive, can reduce the risk of death. Although lactate is currently the most commonly used biomarker to identify sepsis, other biomarkers may help to enhance lactate's effectiveness; these include markers of the hyper-inflammatory phase of sepsis, such as pro-inflammatory cytokines and chemokines; proteins such as C-reactive protein and procalcitonin which are synthesized in response to infection and inflammation; and markers of neutrophil and monocyte activation. Recently, markers of the immunosuppressive phase of sepsis, such as anti-inflammatory cytokines, and alterations of the cell surface markers of monocytes and lymphocytes have been examined. Combinations of pro- and anti-inflammatory biomarkers in a multi-marker panel may help identify patients who are developing severe sepsis before organ dysfunction has advanced too far. Combined with innovative approaches to treatment that target the immunosuppressive phase, these biomarkers may help to reduce the mortality rate associated with severe sepsis which, despite advances in supportive measures, remains high.
Figures
References
-
- Hall MJ, Williams SN, DeFrances CJ, Golosinsky A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. National Center for Health Statistics Data Brief No. 62. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Jun. 2011. http://www.cdc.gov/nchs/data/databriefs/db62.htm Available from: [last accessed 2 Jan 2013]
-
- Wang HE, Shapiro NI, Angus DC, Yealy DM. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007;35:1928–36. - PubMed
-
- Ulevitch RJ, Tobias PS. Recognition of gram-negative bacteria and endotoxin by the innate immune system. Curr Opin Immunol. 1999;11:19–22. - PubMed
-
- Kumar H, Kawai T, Akira S. Pathogen recognition by the innate immune system. Int Rev Immunol. 2011;30:16–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials