

Congenital cytomegalovirus infection: new prospects for prevention and therapy
- PMID: 23481104
- PMCID: PMC3807860
- DOI: 10.1016/j.pcl.2012.12.008
Congenital cytomegalovirus infection: new prospects for prevention and therapy
Abstract
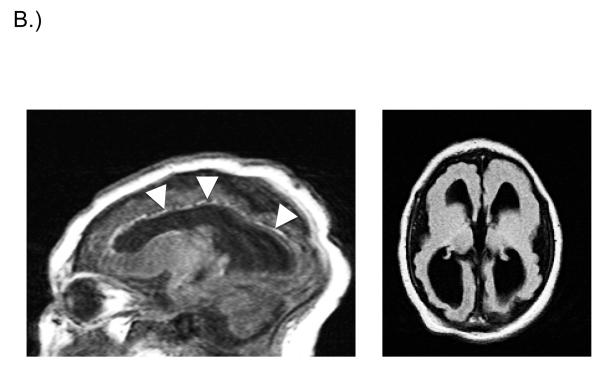
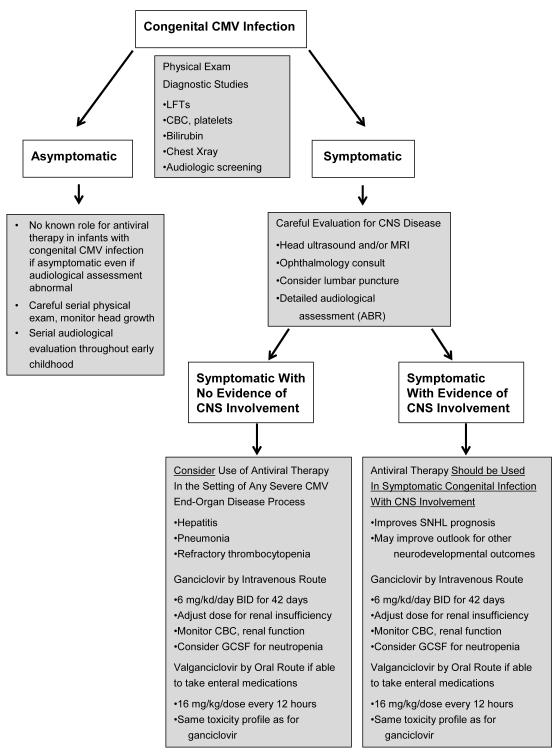
Cytomegalovirus is the commonest congenital viral infection in the developed world, with an overall prevalence of approximately 0.6%. Approximately 10% of congenitally infected infants have signs and symptoms of disease at birth, and these symptomatic infants have a substantial risk of subsequent neurologic sequelae. These include sensorineural hearing loss, mental retardation, microcephaly, development delay, seizure disorders, and cerebral palsy. Antiviral therapy for children with symptomatic congenital cytomegalovirus infection is effective at reducing the risk of long-term disabilities and should be offered to families with affected newborns. An effective preconceptual vaccine against CMV could protect against long-term neurologic sequelae and other disabilities.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures

References
-
- Staras SA, Dollard SC, Radford KW, et al. Seroprevalence of cytomegalovirus infection in the United States, 1988-1994. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2006;43(9):1143–1151. - PubMed
-
- Dollard SC, Grosse SD, Ross DS. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev Med Virol. 2007;17(5):355–363. - PubMed
-
- Kenneson A, Cannon MJ. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev Med Virol. 2007;17(4):253–276. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
