

Minimal clinically important differences of 3 patient-rated outcomes instruments
- PMID: 23481405
- PMCID: PMC3640345
- DOI: 10.1016/j.jhsa.2012.12.032
Minimal clinically important differences of 3 patient-rated outcomes instruments
Abstract
Purpose: Patient-rated instruments are increasingly used to measure orthopedic outcomes. However, the clinical relevance of modest score changes on such instruments is often unclear. This study was designed to define the minimal clinically important differences (MCIDs) of the Disabilities of the Arm, Shoulder, and Hand (DASH), QuickDASH (subset of DASH), and Patient-Rated Wrist Evaluation (PRWE) questionnaires for atraumatic conditions of the hand, wrist, and forearm.
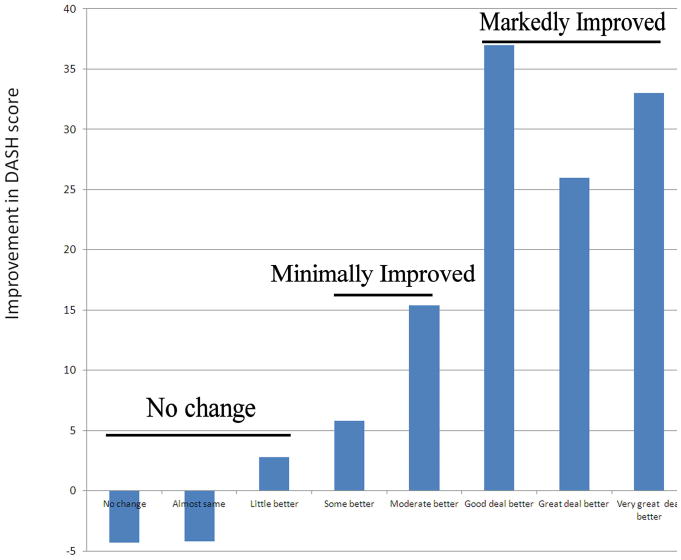
Methods: We prospectively analyzed 102 patients undergoing nonoperative treatment for isolated tendinitis, arthritis, or nerve compression syndromes from the forearm to the hand. By phone, patients completed the DASH, QuickDASH, and PRWE at enrollment and at 2 weeks (n = 78 used in the analysis) and 4 weeks (n = 24 used in the analysis) after initiating treatment. Patients reporting clinical improvement each contributed a single data point categorized as no change (n = 41), minimal improvement (n = 30), or marked improvement (n = 31) via a validated anchor-based approach. We calculated the MCID as the mean change score for each outcome measure in the minimal improvement group.
Results: The MCID (95% confidence interval) for the DASH was 10 (5-15). The MCID for the QuickDASH was 14 (9-20). The MCID was 14 (8-20) for the PRWE. The MCID values were significantly different from changes in these outcome measures at times of either no change or marked improvement. The MCID values positively correlated with baseline outcome measure scores to a greater degree than final outcome measure scores.
Conclusions: Longitudinal changes on the DASH of 10 points, on the QuickDASH of 14 points, and on the PRWE of 14 points represent minimal clinically important changes. We recommend application of these MCID values for group-level analysis when conducting research and interpreting data examining groups of patients as opposed to assessing individual patients. These MCID values may provide a basis for sample size calculations for future investigation using these common patient-rated outcome measures.
Type of study/level of evidence: Diagnostic III.
Copyright © 2013 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4):407–415. - PubMed
-
- Guyatt GH, Osoba D, Wu AW, Wyrwich KW, Norman GR Clinical Significance Consensus Meeting G. Methods to explain the clinical significance of health status measures. Mayo Clin Proc. 2002;77(4):371–383. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
