

MRI-guided intervention for breast lesions using the freehand technique in a 3.0-T closed-bore MRI scanner: feasibility and initial results
- PMID: 23482868
- PMCID: PMC3590327
- DOI: 10.3348/kjr.2013.14.2.171
MRI-guided intervention for breast lesions using the freehand technique in a 3.0-T closed-bore MRI scanner: feasibility and initial results
Abstract
Objective: To report the feasibility of magnetic resonance imaging (MRI)-guided intervention for diagnosing suspicious breast lesions detectable by MRI only, using the freehand technique with a 3.0-T closed-bore MRI scanner.
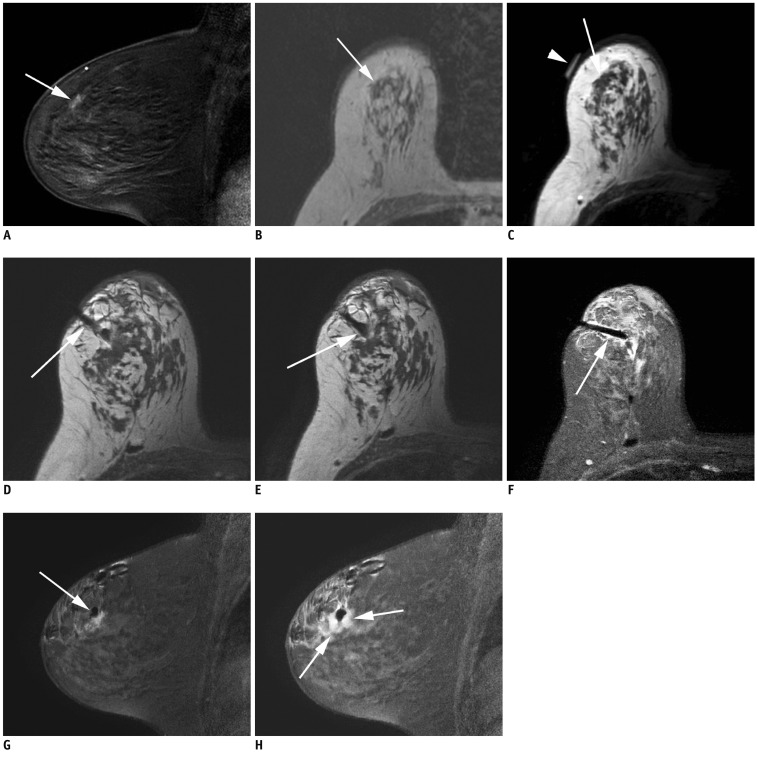
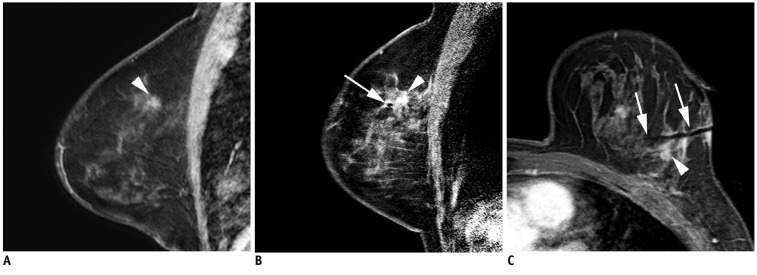
Materials and methods: Five women with 5 consecutive MRI-only breast lesions underwent MRI-guided intervention: 3 underwent MRI-guided needle localization and 2, MRI-guided vacuum-assisted biopsy. The interventions were performed in a 3.0-T closed-bore MRI system using a dedicated phased-array breast coil with the patients in the prone position; the freehand technique was used. Technical success and histopathologic outcome were analyzed.
Results: MRI showed that four lesions were masses (mean size, 11.5 mm; range, 7-18 mm); and 1, a nonmass-like enhancement (maximum diameter, 21 mm). The locations of the lesions with respect to the breast with index cancer were as follows: different quadrant, same breast - 3 cases; same quadrant, same breast - 1 case; and contralateral breast - 1 case. Histopathologic evaluation of the lesions treated with needle localization disclosed perilobular hemangioma, fibrocystic change, and fibroadenomatous change. The lesions treated with vacuum-assisted biopsy demonstrated a radial scar and atypical apocrine hyperplasia. Follow-up MRI after 2-7 months (mean, 4.6 months) confirmed complete lesion removal in all cases.
Conclusion: MRI-guided intervention for breast lesions using the freehand technique with a 3.0-T closed-bore MRI scanner is feasible and accurate for diagnosing MRI-only lesions.
Keywords: Biopsy; Breast neoplasms; Freehand technique; High field; Magnetic resonance imaging; Needle localization.
Figures

Similar articles
-
Targeting difficult accessible breast lesions: MRI-guided needle localization using a freehand technique in a 3.0 T closed bore magnet.Eur J Radiol. 2007 May;62(2):283-8. doi: 10.1016/j.ejrad.2006.12.006. Epub 2007 Jan 10. Eur J Radiol. 2007. PMID: 17218074
-
Freehand MRI-guided preoperative needle localization of breast lesions after MRI-guided vacuum-assisted core needle biopsy without marker placement.J Magn Reson Imaging. 2010 Jul;32(1):101-9. doi: 10.1002/jmri.22148. J Magn Reson Imaging. 2010. PMID: 20575077
-
MR imaging-guided 10-gauge vacuum-assisted breast biopsy: histological characterisation.Radiol Med. 2008 Sep;113(6):830-40. doi: 10.1007/s11547-008-0289-y. Epub 2008 Jul 5. Radiol Med. 2008. PMID: 18633687 English, Italian.
-
Breast Biopsies Under Magnetic Resonance Imaging Guidance: Challenges of an Essential but Imperfect Technique.Curr Probl Diagn Radiol. 2016 May-Jun;45(3):193-204. doi: 10.1067/j.cpradiol.2015.07.002. Epub 2015 Jul 10. Curr Probl Diagn Radiol. 2016. PMID: 26272705 Review.
-
Interventional MRI of the breast: lesion localisation and biopsy.Eur Radiol. 2000;10(1):36-45. doi: 10.1007/s003300050005. Eur Radiol. 2000. PMID: 10663716 Review.
Cited by
-
Is there a Role for Contrast-enhanced Ultrasound in the Detection and Biopsy of MRI Only Visible Breast Lesions?Radiol Oncol. 2017 Nov 29;51(4):386-392. doi: 10.1515/raon-2017-0049. eCollection 2017 Dec. Radiol Oncol. 2017. PMID: 29333116 Free PMC article.
-
Initial experience with magnetic resonance-guided vacuum-assisted biopsy in korean women with breast cancer.J Breast Cancer. 2014 Sep;17(3):270-8. doi: 10.4048/jbc.2014.17.3.270. Epub 2014 Sep 30. J Breast Cancer. 2014. PMID: 25320626 Free PMC article.
References
-
- Orel SG, Schnall MD, LiVolsi VA, Troupin RH. Suspicious breast lesions: MR imaging with radiologic-pathologic correlation. Radiology. 1994;190:485–493. - PubMed
-
- Stomper PC, Herman S, Klippenstein DL, Winston JS, Edge SB, Arredondo MA, et al. Suspect breast lesions: findings at dynamic gadolinium-enhanced MR imaging correlated with mammographic and pathologic features. Radiology. 1995;197:387–395. - PubMed
-
- Boné B, Aspelin P, Bronge L, Isberg B, Perbeck L, Veress B. Sensitivity and specificity of MR mammography with histopathological correlation in 250 breasts. Acta Radiol. 1996;37:208–213. - PubMed
-
- Daniel BL, Yen YF, Glover GH, Ikeda DM, Birdwell RL, Sawyer-Glover AM, et al. Breast disease: dynamic spiral MR imaging. Radiology. 1998;209:499–509. - PubMed
-
- Kuhl CK, Elevelt A, Leutner CC, Gieseke J, Pakos E, Schild HH. Interventional breast MR imaging: clinical use of a stereotactic localization and biopsy device. Radiology. 1997;204:667–675. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
