

The clinical implications of elevated blood metal ion concentrations in asymptomatic patients with MoM hip resurfacings: a cohort study
- PMID: 23482990
- PMCID: PMC3612810
- DOI: 10.1136/bmjopen-2012-001541
The clinical implications of elevated blood metal ion concentrations in asymptomatic patients with MoM hip resurfacings: a cohort study
Erratum in
-
Correction.BMJ Open. 2013 May 9;3(5):e001541corr1. doi: 10.1136/bmjopen-2012-001541corr1. BMJ Open. 2013. PMID: 23667157 Free PMC article. No abstract available.
Abstract
Objective: To determine whether elevated blood cobalt (Co) concentrations are associated with early failure of metal-on-metal (MoM) hip resurfacings secondary to adverse reaction to metal debris (ARMD).
Design: Cohort study.
Setting: Single centre orthopaedic unit.
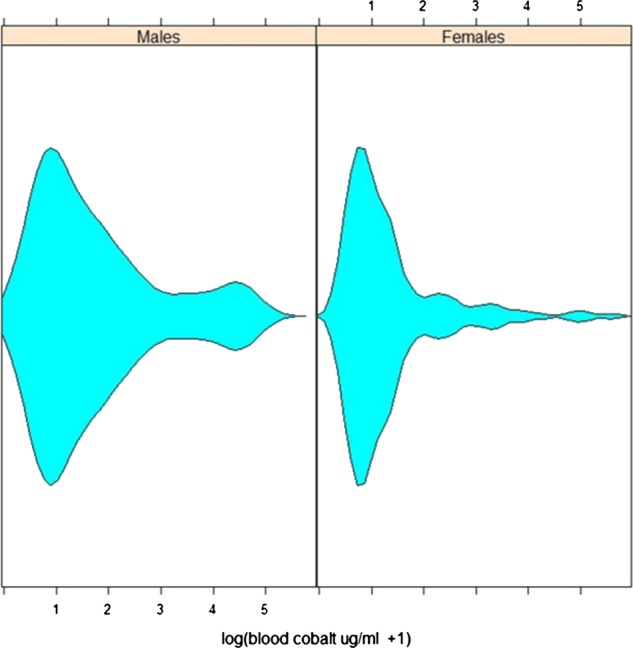
Participants: Following the identification of complications potentially related to metal wear debris, a blood metal ion screening programme was instigated at our unit in 2007 for all patients with Articular Surface Replacement (ASR) and Birmingham MoM hip resurfacings. Patients were followed annually unless symptoms presented earlier. Symptomatic patients were investigated with ultrasound scan and joint aspiration. The clinical course of all 278 patients with 'no pain' or 'slight/occasional' pain and a Harris Hip Score greater than or equal to 95 at the time of venesection were documented. A retrospective analysis was subsequently conducted using mixed effect modelling to investigate the temporal pattern of blood Co levels in the patients and survival analysis to investigate the potential role of case demographics and blood Co levels as risk factors for subsequent failure secondary to ARMD.
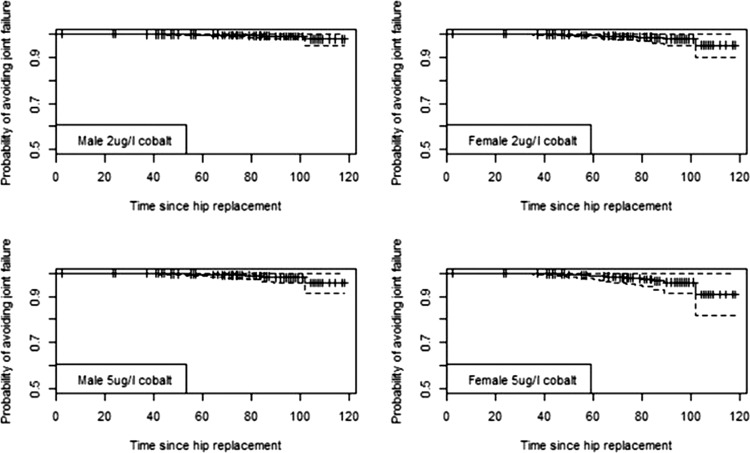
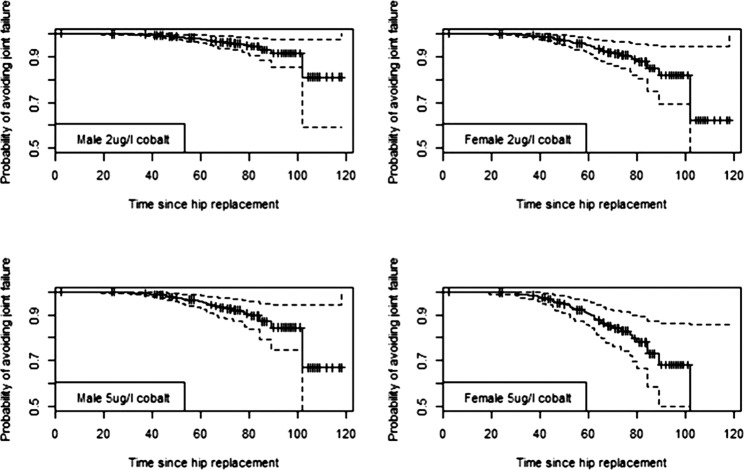
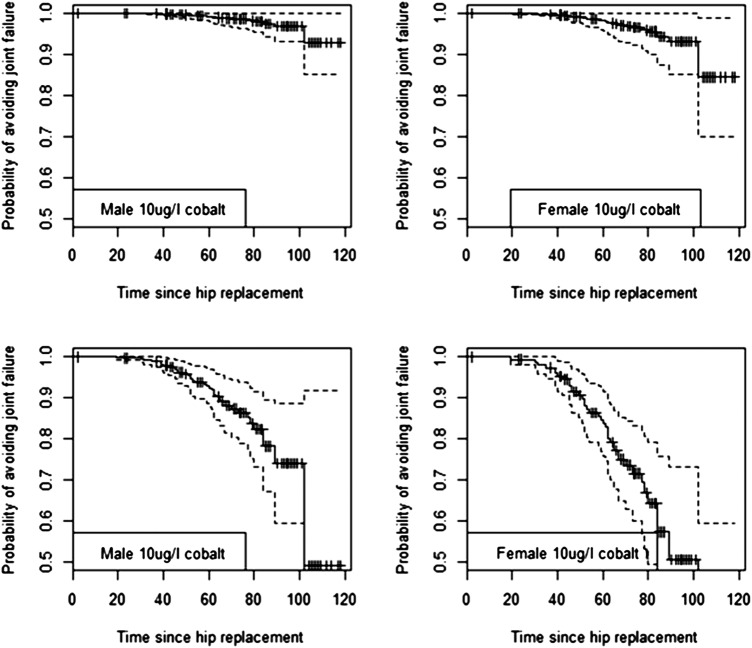
Results: Blood Co concentration was a positive and significant risk factor (z=8.44, p=2×10(-16)) for joint failure, as was the device, where the Birmingham Hip Resurfacing posed a significantly reduced risk for revision by 89% (z=-3.445, p=0.00005 (95% CI on risk 62 to 97)). Analysis using Cox-proportional hazards models indicated that men had a 66% lower risk of joint failure than women (z=-2.29419, p=0.0218, (95% CI on risk reduction 23 to 89)).
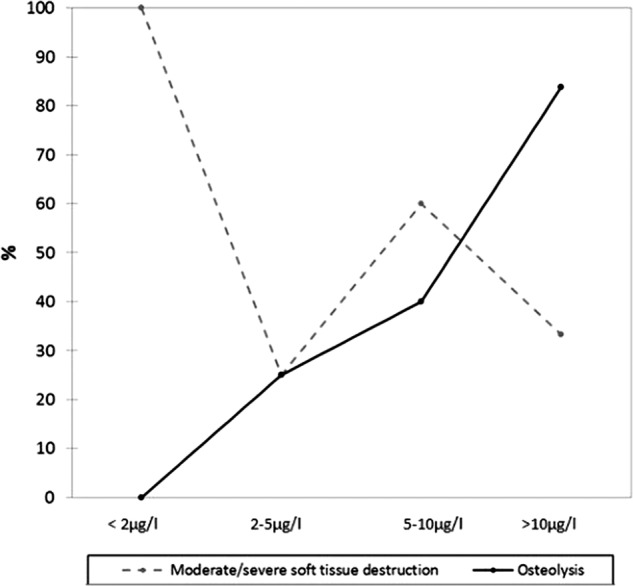
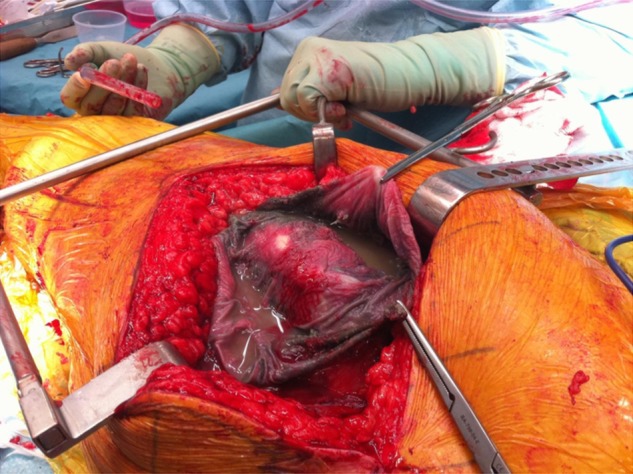
Conclusions: The results suggest that elevated blood metal ion concentrations are associated with early failure of MoM devices secondary to adverse reactions to metal debris. Co concentrations greater than 20 µg/l are frequently associated with metal staining of tissues and the development of osteolysis. Development of soft tissue damage appears to be more complex with females and patients with ASR devices seemingly more at risk when exposed to equivalent doses of metal debris.
Figures

References
-
- McMinn D, Treacy R, Lin K, et al. Metal on metal surface replacement of the hip. Experience of the McMinn prothesis. Clin Orthop Relat Res 1996;89–98 - PubMed
-
- Treacy RB, McBryde CW, Shears E, et al. Birmingham hip resurfacing: a minimum follow-up of ten years. J Bone Joint Surg (Br) 2011;93:27–33 - PubMed
-
- Coulter G, Young DA, Dalziel RE, et al. Birmingham hip resurfacing at a mean of ten years: results from an independent centre. J Bone Joint Surg (Br) 2012;94:315–21 - PubMed
-
- Delaunay C, Petit I, Learmonth ID, et al. Metal-on-metal bearings total hip arthroplasty: the cobalt and chromium ions release concern. Orthop Traumatol Surg Res 2010;96:894–904 - PubMed
-
- Jones DA, Lucas HK, O'Driscoll M, et al. Cobalt toxicity after McKee hip arthroplasty. J Bone Joint Surg (Br) 1975; 57-B:289–96 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources