

The efficacy and safety of linezolid and glycopeptides in the treatment of Staphylococcus aureus infections
- PMID: 23484002
- PMCID: PMC3590119
- DOI: 10.1371/journal.pone.0058240
The efficacy and safety of linezolid and glycopeptides in the treatment of Staphylococcus aureus infections
Abstract
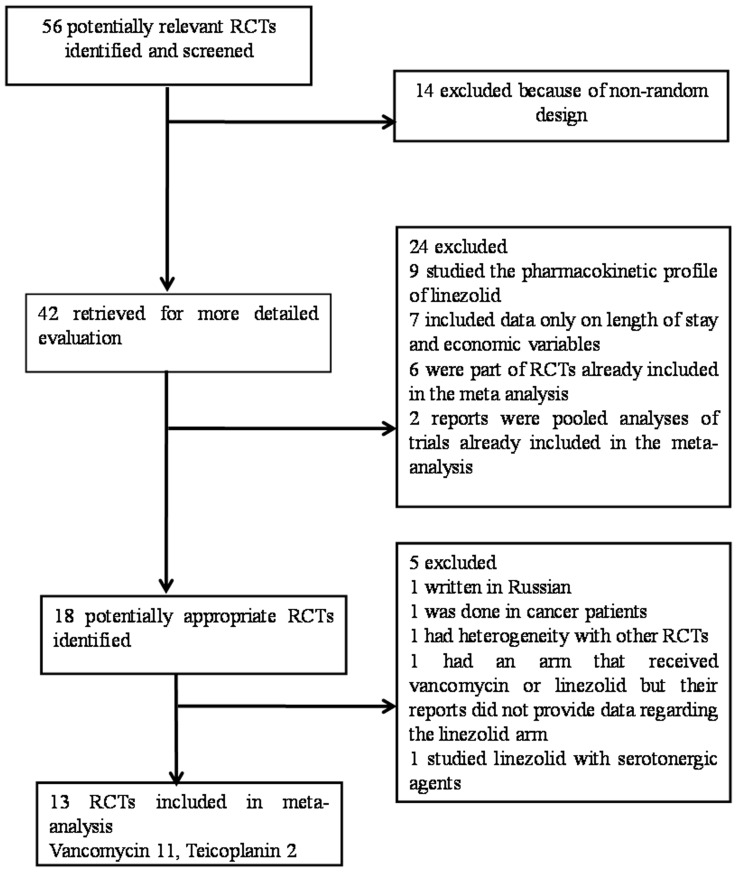
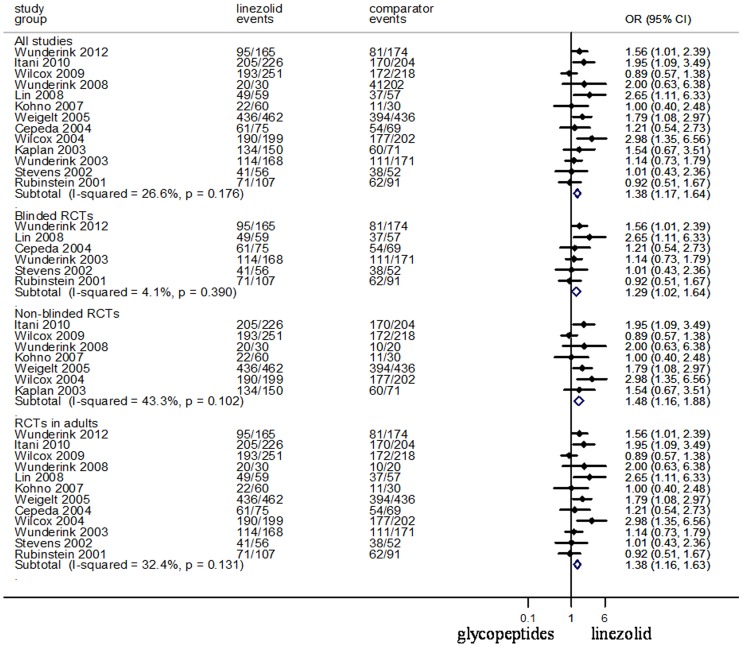
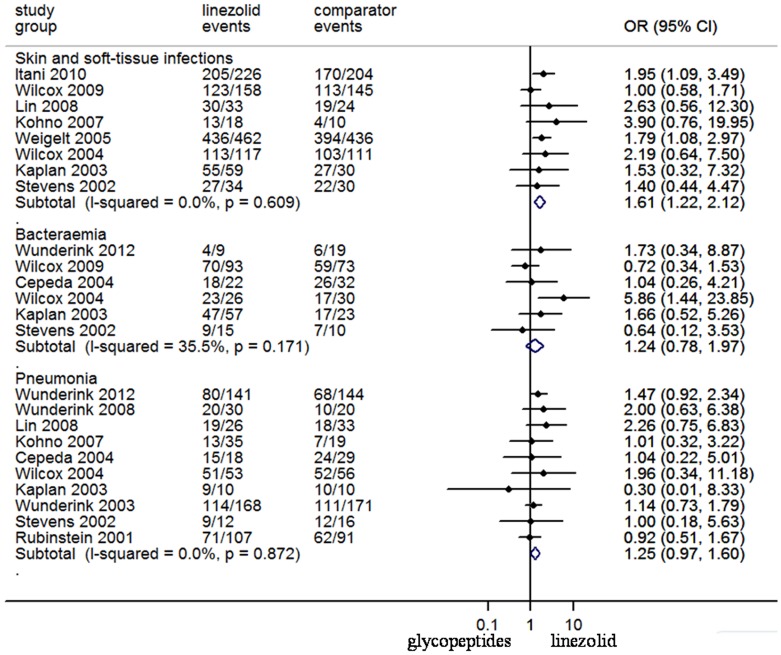
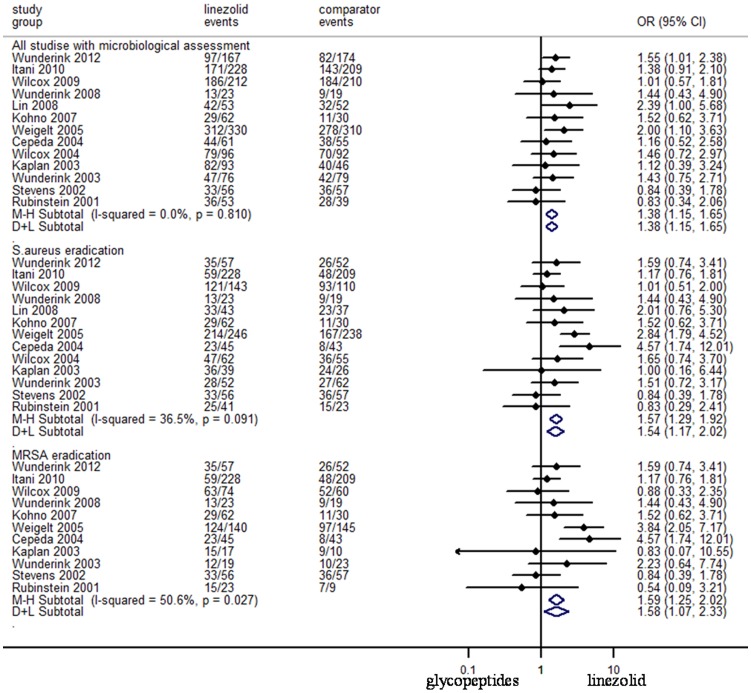
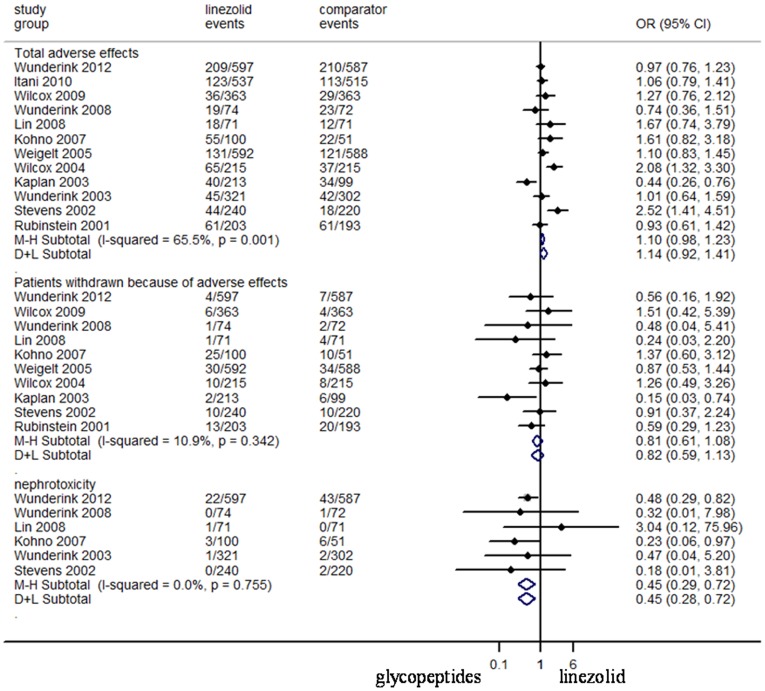
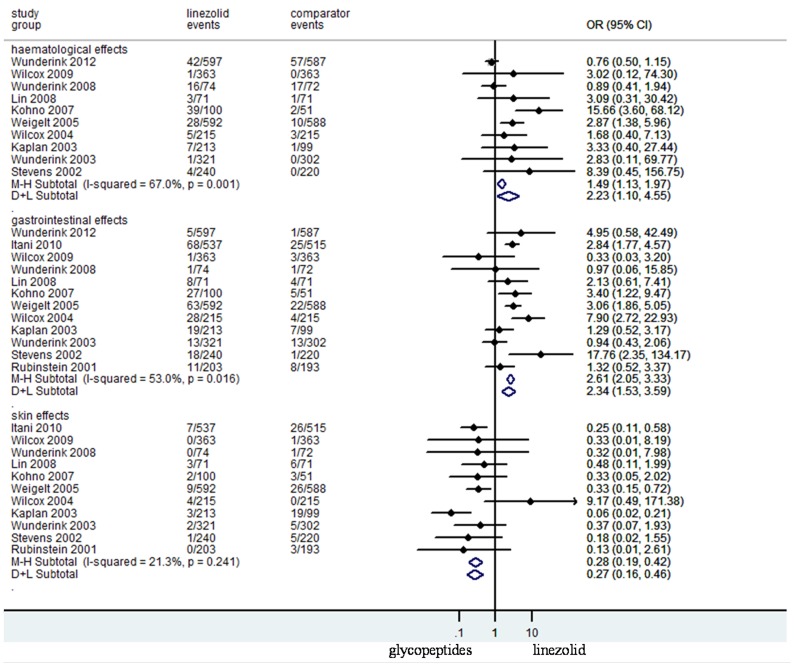
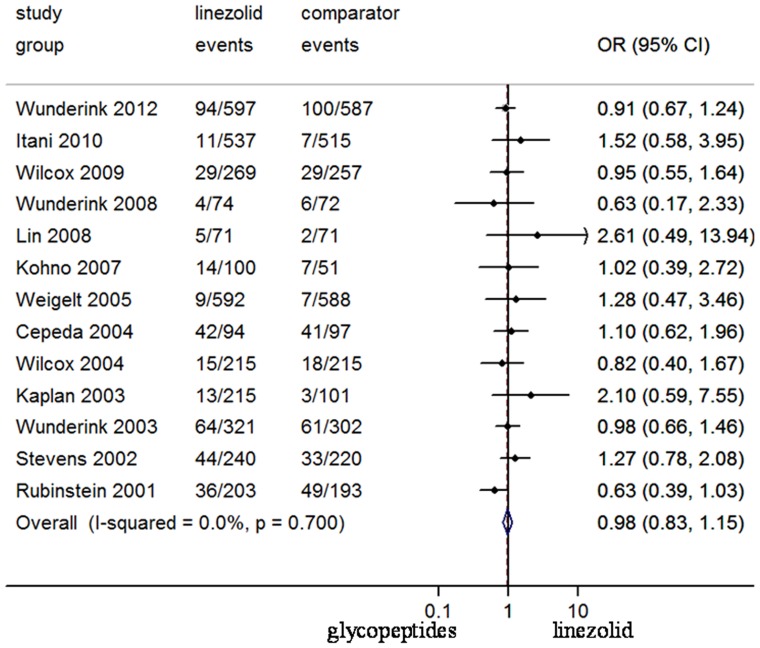
To assess the effectiveness and safety of linezolid in comparison with glycopeptides (vancomycin and teicoplanin) for the treatment of Staphylococcus aureus infections, we conducted a meta-analysis of relevant randomized controlled trials. A thorough search of Pubmed and other databases was performed. Thirteen trials on 3863 clinically assessed patients were included. Linezolid was slightly more effective than glycopeptides in the intent-to-treat population (odds ratio [OR], 1.05; 95% confidence interval [CI], 1.01-1.10), was more effective in clinically assessed patients (OR 95% CI: 1.38, 1.17-1.64) and in all microbiologically assessed patients (OR 95% CI: 1.38, 1.15-1.65). Linezolid was associated with better treatment in skin and soft-tissue infections (SSTIs) patients (OR 95% CI: 1.61, 1.22-2.12), but not in bacteraemia (OR 95% CI: 1.24, 0.78-1.97) or pneumonia (OR 95% CI: 1.25, 0.97-1.60) patients. No difference of mortality between linezolid and glycopeptides was seen in the pooled trials (OR 95% CI: 0.98, 0.83-1.15). While linezolid was associated with more haematological (OR 95% CI: 2.23, 1.07-4.65) and gastrointestinal events (OR 95% CI: 2.34, 1.53-3.59), a significantly fewer events of skin adverse effects (OR 95% CI: 0.27, 0.16-0.46) and nephrotoxicity (OR 95% CI: 0.45, 0.28-0.72) were recorded in linezolid. Based on the analysis of the pooled data of randomized control trials, linezolid should be a better choice for treatment of patients with S. aureus infections, especially in SSTIs patients than glycopeptides. However, when physicians choose to use linezolid, risk of haematological and gastrointestinal events should be taken into account according to the characteristics of the specific patient populations.
Conflict of interest statement
Figures
References
-
- Herold BC, Immergluck LC, Maranan MC, Lauderdale DS, Gaskin RE, et al. (1998) Community- acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA 279: 593–598. - PubMed
-
- Vardakas KZ, Matthaiou DK, Falagas ME (2009) Incidence, characteristics and outcomes of patients with severe community acquired-MRSA pneumonia. Eur Respir J 34: 1148–1158. - PubMed
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, et al. (2003) Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis 36: 53–59. - PubMed
-
- Moet GJ, Jones RN, Biedenbach DJ, Stilwell MG, Fritsche TR (2007) Contemporary causes of skin and soft tissue infections in North America, Latin America, and Europe: report from the SENTRY Antimicrobial Surveillance Program (1998–2004). Diagn Microbiol Infect Dis 57: 7–13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
