

Long-term outcomes in elderly survivors of in-hospital cardiac arrest
- PMID: 23484828
- PMCID: PMC3652256
- DOI: 10.1056/NEJMoa1200657
Long-term outcomes in elderly survivors of in-hospital cardiac arrest
Abstract
Background: Little is known about the long-term outcomes in elderly survivors of in-hospital cardiac arrest. We determined rates of long-term survival and readmission among survivors of in-hospital cardiac arrest and examined whether these outcomes differed according to demographic characteristics and neurologic status at discharge.
Methods: We linked data from a national registry of inpatient cardiac arrests with Medicare files and identified 6972 adults, 65 years of age or older, who were discharged from the hospital after surviving an in-hospital cardiac arrest between 2000 and 2008. Predictors of 1-year survival and of readmission to the hospital were examined.
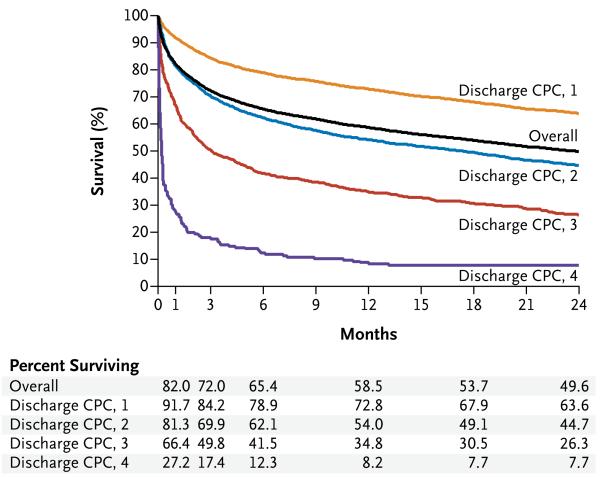
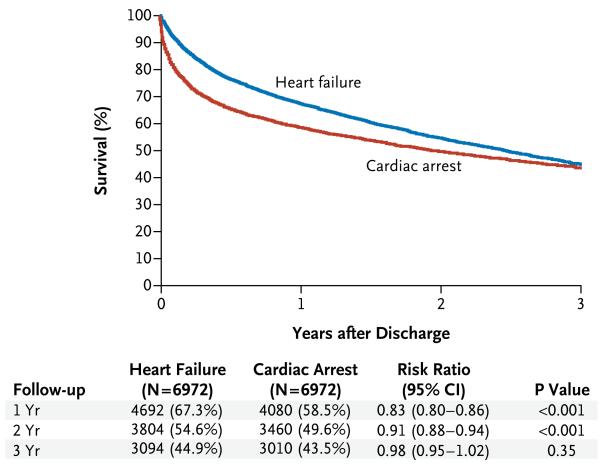
Results: One year after hospital discharge, 58.5% of the patients were alive, and 34.4% had not been readmitted to the hospital. The risk-adjusted rate of 1-year survival was lower among older patients than among younger patients (63.7%, 58.6%, and 49.7% among patients 65 to 74, 75 to 84, and ≥85 years of age, respectively; P<0.001), among men than among women (58.6% vs. 60.9%, P=0.03), and among black patients than among white patients (52.5% vs. 60.4%, P=0.001). The risk-adjusted rate of 1-year survival was 72.8% among patients with mild or no neurologic disability at discharge, as compared with 61.1% among patients with moderate neurologic disability, 42.2% among those with severe neurologic disability, and 10.2% among those in a coma or vegetative state (P<0.001 for all comparisons). Moreover, 1-year readmission rates were higher among patients who were black, those who were women, and those who had substantial neurologic disability (P<0.05 for all comparisons). These differences in survival and readmission rates persisted at 2 years. At 3 years, the rate of survival among survivors of in-hospital cardiac arrest was similar to that of patients who had been hospitalized with heart failure and were discharged alive (43.5% and 44.9%, respectively; risk ratio, 0.98; 95% confidence interval, 0.95 to 1.02; P=0.35).
Conclusions: Among elderly survivors of in-hospital cardiac arrest, nearly 60% were alive at 1 year, and the rate of 3-year survival was similar to that among patients with heart failure. Survival and readmission rates differed according to the demographic characteristics of the patients and neurologic status at discharge. (Funded by the American Heart Association and the National Heart, Lung, and Blood Institute.).
Figures
Comment in
-
Elderly in-hospital cardiac arrest patients who are resuscitated with neurological recovery experience favourable long-term survival similar to non-arrest heart failure patients.Evid Based Med. 2013 Dec;18(6):227-8. doi: 10.1136/eb-2013-101351. Epub 2013 May 15. Evid Based Med. 2013. PMID: 23676758 No abstract available.
-
Long-term outcomes in elderly survivors of cardiac arrest.N Engl J Med. 2013 Jun 20;368(25):2438-9. doi: 10.1056/NEJMc1305198. N Engl J Med. 2013. PMID: 23782192 No abstract available.
-
Long-term outcomes in elderly survivors of cardiac arrest.N Engl J Med. 2013 Jun 20;368(25):2437-8. doi: 10.1056/NEJMc1305198. N Engl J Med. 2013. PMID: 23782193 No abstract available.
-
Long-term outcomes in elderly survivors of cardiac arrest.N Engl J Med. 2013 Jun 20;368(25):2438. doi: 10.1056/NEJMc1305198. N Engl J Med. 2013. PMID: 23782194 No abstract available.
References
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. - PubMed
-
- Chan PS, Krumholz HM, Nichol G, Nallamothu BK. Delayed time to defibrillation after in-hospital cardiac arrest. N Engl J Med. 2008;358:9–17. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295:50–7. - PubMed
-
- Kalbag A, Kotyra Z, Richards M, Spearpoint K, Brett SJ. Long-term survival and residual hazard after in-hospital cardiac arrest. Resuscitation. 2006;68:79–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical