

Evolving management of symptomatic chronic subdural hematoma: experience of a single institution and review of the literature
- PMID: 23485050
- PMCID: PMC4564993
- DOI: 10.1179/1743132813Y.0000000166
Evolving management of symptomatic chronic subdural hematoma: experience of a single institution and review of the literature
Abstract
Objective: Chronic subdural hematoma (cSDH) has an increasing incidence and results in high morbidity and mortality. We review here the 10-year experience of a single institution and the literature regarding the treatment and major associations of cSDH.
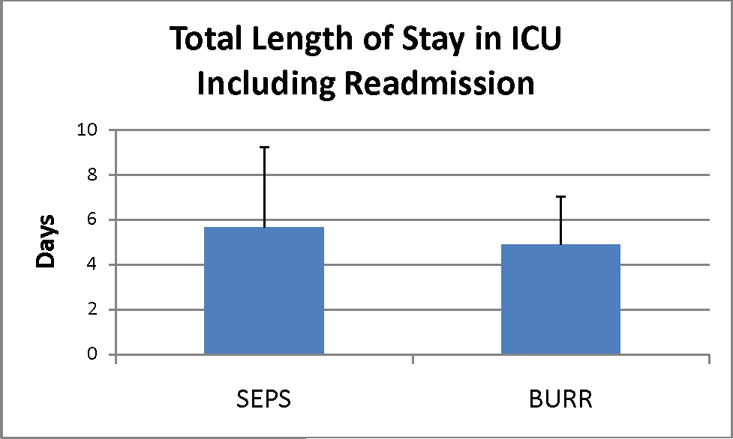
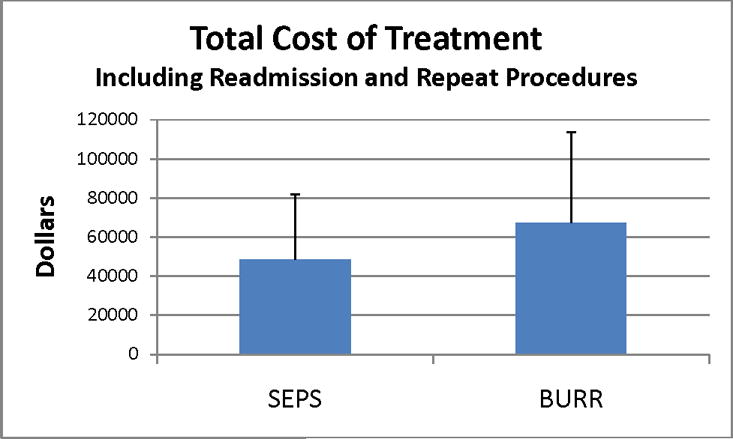
Methods: We retrospectively reviewed all cSDHs surgically treated from 2000 to 2010 in the New York Harbor Health Care System to evaluate the duration from admission to treatment, type of treatment, length of stay (LOS) in critical care, LOS in the hospital, and recurrence. The literature was reviewed with regards to incidence, associations, and treatment of cSDH.
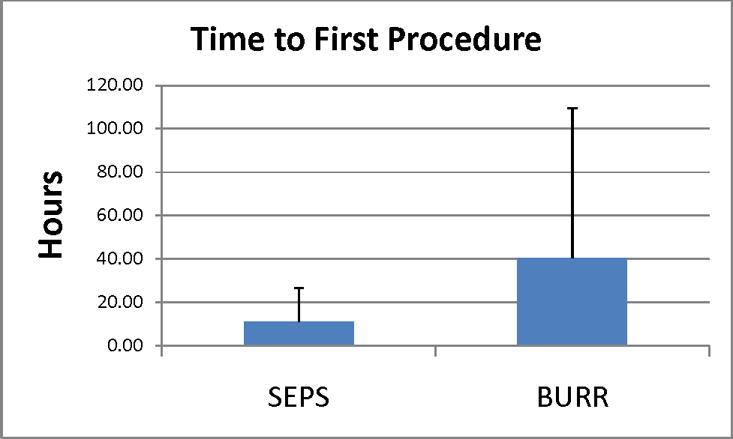
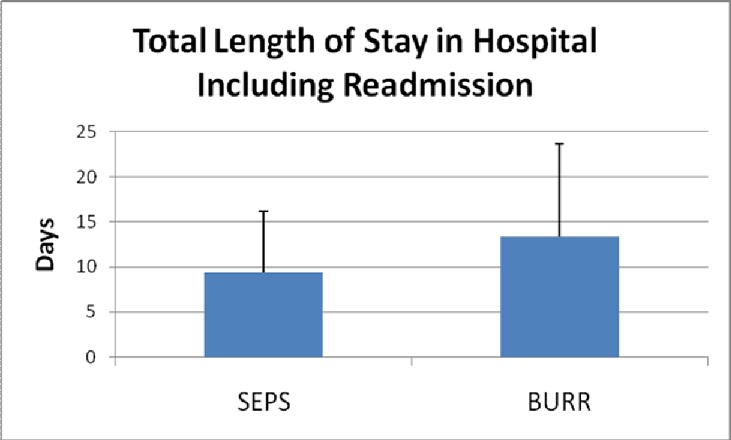
Results: From 2000 to 2008, 44 patients were treated with burr holes (BHs). From 2008 to 2010, 29 patients were treated with twist-drill evacuation (subdural evacuating port system, SEPS). Four patients from each group were readmitted for reoperation (9% vs 14%; P = 0.53). The average time to intervention for SEPS (11.2 ± 15.3 hours) was faster than for BHs (40.3 ± 69.1 hours) (P = 0.02). The total hospital LOS was shorter for SEPS (9.3 ± 6.8 days) versus BHs (13.4 ± 10.2 days) (P = 0.04); both were significantly longer than for a brain tumor patient undergoing craniotomy (7.0 ± 0.5 days, n = 94, P < 0.01).
Conclusion: Despite decreasing LOSs as treatment for cSDH evolved from BHs to SEPS, the LOS for a cSDH is still longer than that of a patient undergoing craniotomy for brain tumor. We noted 11% recurrence in our series of patients, which included individuals who recurred as late as 3 years after initial diagnosis.
Figures
References
-
- Filippini G. Epidemiology of primary central nervous system tumors. Handb Clin Neurol. 2012;104:3–22. - PubMed
-
- Gavrilovic IT, Posner JB. Brain metastases: Epidemiology and pathophysiology. J Neurooncol. 2005;75:5–14. - PubMed
-
- Kudo H, Kuwamura K, Izawa I, Sawa H, Tamaki N. Chronic subdural hematoma in elderly people: Present status on awaji island and epidemiological prospect. Neurol Med Chir (Tokyo) 1992;32:207–9. - PubMed
-
- Center PR. Aging of america. 2011 http://www.prcdc.org/300million/The_Aging_of_America/.
-
- Foelholm R, Waltimo O. Epidemiology of chronic subdural haematoma. Acta Neurochir (Wien) 1975;32:247–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical