

Neuropathic pain in the community: more under-treated than refractory?
- PMID: 23485369
- PMCID: PMC3630326
- DOI: 10.1016/j.pain.2012.12.022
Neuropathic pain in the community: more under-treated than refractory?
Abstract
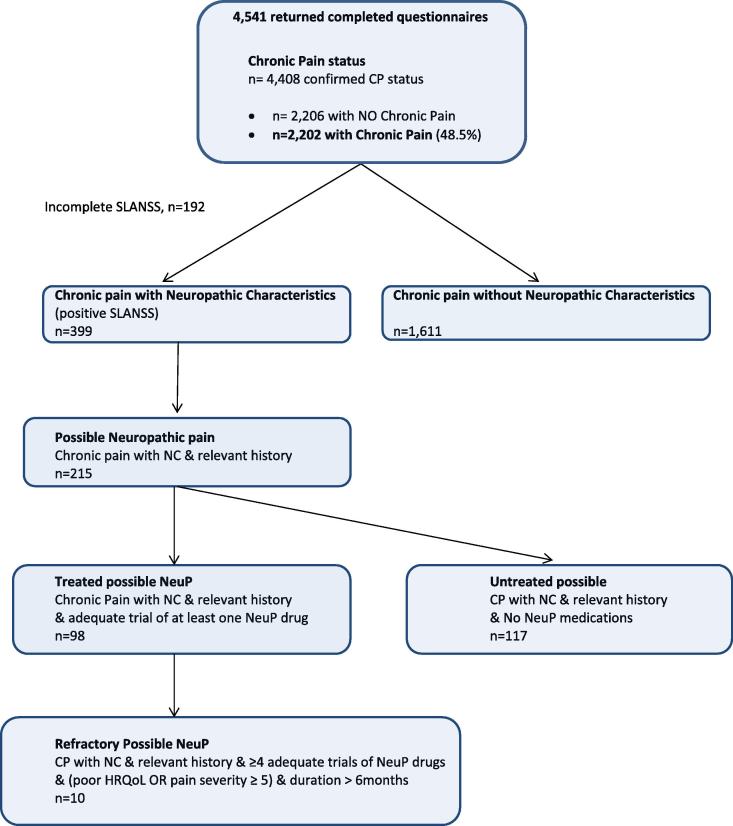
Best current estimates of neuropathic pain prevalence come from studies using screening tools detecting pain with probable neuropathic features; the proportion experiencing significant, long-term neuropathic pain, and the proportion not responding to standard treatment are unknown. These "refractory" cases are the most clinically important to detect, being the most severe, requiring specialist treatment. The aim of this study was to estimate the proportion of neuropathic pain in the population that is "refractory," and to quantify associated clinical and demographic features. We posted self-administered questionnaires to 10,000 adult patients randomly selected from 10 general practitioner practices in 5 UK locations. The questionnaire contained chronic pain identification and severity questions, cause of pain, SF-12, EQ-5D, S-LANSS (Self-administered Leeds Assessment of Neuropathic Signs and Symptoms), PSEQ (Pain Self-Efficacy Questionnaire), use of neuropathic pain medications, and health care utilisation. These data were combined to determine the presence and characteristics of "refractory" neuropathic pain according to the defining features identified by a Delphi survey of international experts. Graded categories of chronic pain with and without neuropathic characteristics were generated, incorporating the refractory criteria. Completed questionnaires were returned by 4451 individuals (response rate 47%); 399 had "chronic pain with neuropathic characteristics" (S-LANSS positive, 8.9% of the study sample); 215 (53.9%) also reported a positive relevant history ("Possible neuropathic pain"); and 98 (4.5% of all Chronic Pain) also reported an "adequate" trial of at least one neuropathic pain drug ("Treated possible neuropathic pain"). The most refractory cases were associated with dramatically poorer physical and mental health, lower pain self-efficacy, higher pain intensity and pain-related disability, and greater health care service use.
Copyright © 2013 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Attal N., Cruccu G., Baron R., Haanpaa M., Hansson P., Jensen T.S., Nurmikko T. European federation of neurological societies. EFNS guidelines on the pharmacological treatment of neuropathic pain. Eur J Neurol. 2010 revision;2010:e1113–e1188. - PubMed
-
- Attal N., Lanteri-Minet M., Laurent B., Fermanian J., Bouhassira D. The specific disease burden of neuropathic pain: results of a French nationwide survey. PAIN®. 2011;152:2836–2843. - PubMed
-
- Bennett M.I., Smith B.H., Torrance N., Lee A.J. Can pain be more or less neuropathic? Comparison of symptom assessment tools with ratings of certainty by clinicians. PAIN®. 2006;122:289–294. - PubMed
-
- Bennett M.I., Smith B.H., Torrance N., Potter J. The S-LANSS score for identifying pain of predominantly neuropathic origin: validation for use in clinical and postal research. J Pain. 2005;6:149–158. - PubMed
-
- Bouhassira D., Chassany O., Gaillat J., Hanslik T., Launay O., Mann C., Rabaud C., Rogeaux O., Strady C. Patient perspective on herpes zoster and its complications: an observational prospective study in patients aged over 50 years in general practice. PAIN®. 2012;153:342–349. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
