

Markers of intestinal inflammation, not bacterial burden, correlate with clinical outcomes in Clostridium difficile infection
- PMID: 23487367
- PMCID: PMC3707425
- DOI: 10.1093/cid/cit147
Markers of intestinal inflammation, not bacterial burden, correlate with clinical outcomes in Clostridium difficile infection
Abstract
Background: Clostridium difficile is a leading hospital-acquired infection. Many patients remain symptomatic for several days on appropriate antibiotic therapy. To assess the contribution of ongoing infection vs persistent inflammation, we examined the correlation between fecal cytokine levels, fecal C. difficile burden, and disease outcomes in C. difficile infection (CDI).
Methods: We conducted a prospective cohort study in Barnes Jewish Hospital between June 2011 and May 2012 of hospitalized adults with CDI. We determined fecal interleukin 8 (IL-8) and lactoferrin protein concentrations by enzyme immunoassay. We used real-time polymerase chain reaction (PCR) to measure relative fecal IL-8 and CXCL-5 RNA transcript abundances, and quantitative PCR to enumerate C. difficile burden.
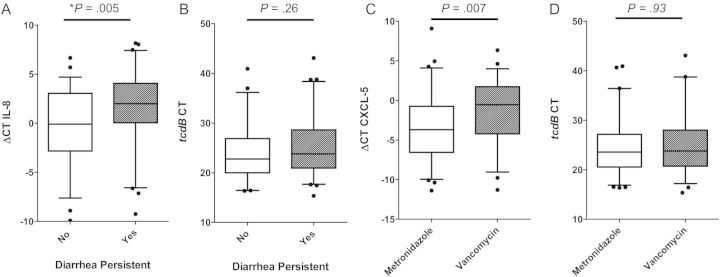
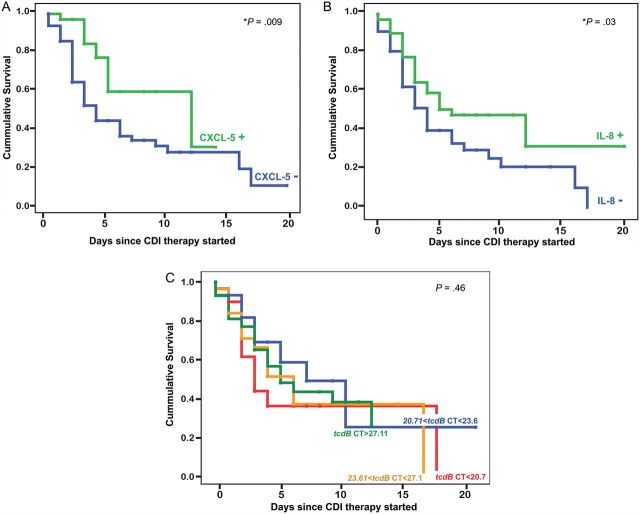
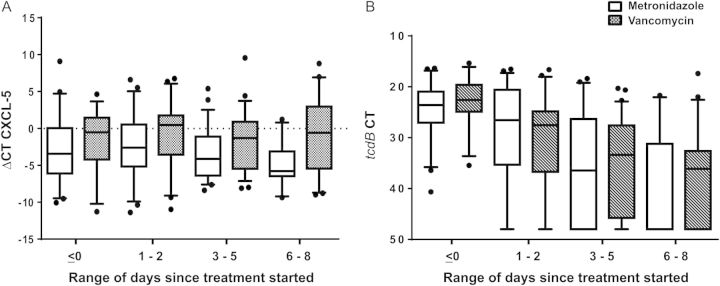
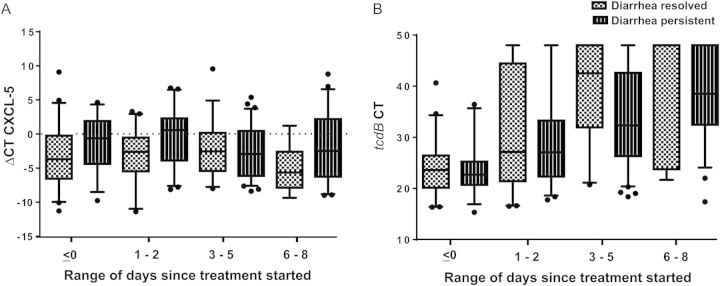
Results: Of 120 study subjects, 101 (84%) were started on metronidazole, and 33 of those (33%) were subsequently given vancomycin. Sixty-two (52%) patients had diarrhea persistent for 5 or more days after starting CDI therapy. Initial fecal CXCL-5 messenger RNA (mRNA), IL-8 mRNA, and IL-8 protein correlated with persistent diarrhea and use of vancomycin. Time to diarrhea resolution was longer in patients with elevated fecal cytokines at diagnosis. Fecal cytokines were more sensitive than clinical severity scores in identifying patients at risk of treatment failure. Clostridium difficile burden did not correlate with any measure of illness or outcome at any point, and decreased equally with metronidazole and vancomycin.
Conclusions: Persistent diarrhea in CDI correlates with intestinal inflammation and not fecal pathogen burden. These findings suggest that modulation of host response, rather than adjustments to antimicrobial regimens, might be a more effective approach to patients with unremitting disease.
Keywords: CXCL-5; Clostridium difficile; IL-8; cytokines; inflammation.
Figures
Comment in
-
The role of gut inflammation in recurrent Clostridium difficile-associated disease.Clin Infect Dis. 2013 Jun;56(12):1722-3. doi: 10.1093/cid/cit151. Epub 2013 Mar 13. Clin Infect Dis. 2013. PMID: 23487370 No abstract available.
References
-
- McFarland LV. Antibiotic-associated diarrhea: epidemiology, trends and treatment. Future Microbiol. 2008;3:563–78. - PubMed
-
- Johnson S, Gerding DN. Clostridium difficile–associated diarrhea. Clin Infect Dis. 1998;26:1027–34. quiz 35–6. - PubMed
-
- Dubberke ER, Reske KA, Yan Y, Olsen MA, McDonald LC, Fraser VJ. Clostridium difficile–associated disease in a setting of endemicity: identification of novel risk factors. Clin Infect Dis. 2007;45:1543–9. - PubMed
-
- DuPont HL, Garey K, Caeiro JP, Jiang ZD. New advances in Clostridium difficile infection: changing epidemiology, diagnosis, treatment and control. Current Opinion Infect Dis. 2008;21:500–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
