

The transurethral suprapubic endo-cystostomy (T-SPeC): a novel suprapubic catheter insertion device
- PMID: 23488708
- PMCID: PMC3708625
- DOI: 10.1089/end.2013.0053
The transurethral suprapubic endo-cystostomy (T-SPeC): a novel suprapubic catheter insertion device
Abstract
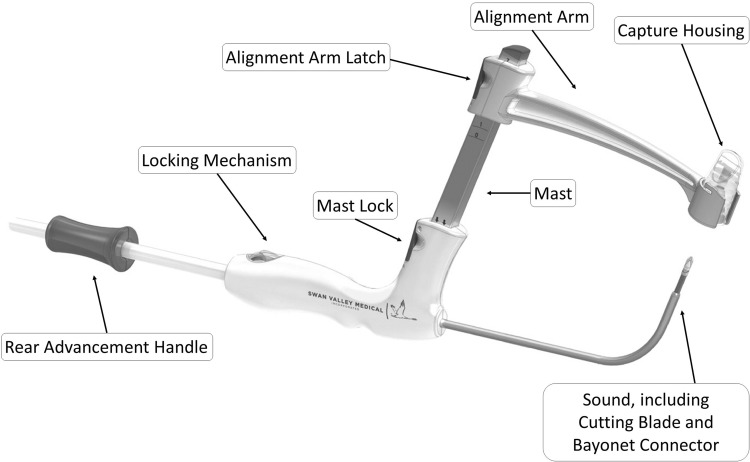
Background and purpose: Current methods of suprapubic cystostomy (SPC) catheter insertion may be difficult for patients in poor health and can result in significant morbidity and mortality. These include a highly invasive open procedure, as well as the use of the percutaneous trocar punch methods, commonly associated with short-term SPC. We present the first human experience with the Transurethral Suprapubic endo-Cystostomy (T-SPeC(®)) device, a novel disposable device used for introducing a suprapubic catheter via a retrourethral (inside-to-out) approach similar to the Lowsley technique.
Patients and methods: Four men at St. Mary's General Hospital in Kitchener Ontario, Canada, received the T-SPeC device (model T7) under general anesthesia.
Results: Patients had no complications from catheterization using the T-SPeC T7 Surgical System. The mean surgical time of the four procedures was 9.7 minutes, with a range of 7.9 to 13.5 minutes, including instrument preparation and cystoscopy. All four procedures were highly accurate and rapid. There were no complications and minimal blood loss from the procedure.
Conclusions: We found that the T-SPeC device allows for efficient and safe insertion of a suprapubic catheter in an outpatient setting and may be a useful addition to the urologic armamentarium. The T-SPeC Surgical System facilitates rapid and precise suprapubic catheter placement.
Figures


References
-
- Zeidman EJ. Chiang H. Alarcon A. Raz S. Suprapubic cystostomy using Lowsley retractor. Urology. 1988;32:54–55. - PubMed
-
- Edokpolo LU. Foster HE., Jr Suprapubic cystostomy for neurogenic bladder using Lowsley retractor method: A procedure revisited. Urology. 2011;78:1196–1198. - PubMed
-
- Harrison SC. Lawrence WT. Morley R, et al. British Association of Urological Surgeons' suprapubic catheter practice guidelines. BJU Int. 2011;107:77–85. - PubMed
-
- Irby PB., 3rd Stoller ML. Percutaneous suprapubic cystostomy. J Endourol. 1993;7:125–130. - PubMed
-
- Krane LS. Bhandari M. Peabody JO. Menon M. Impact of percutaneous suprapubic tube drainage on patient discomfort after radical prostatectomy. Eur Urol. 2009;56:325–330. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
