

PDE3, but not PDE4, reduces β₁ - and β₂-adrenoceptor-mediated inotropic and lusitropic effects in failing ventricle from metoprolol-treated patients
- PMID: 23489141
- PMCID: PMC3682702
- DOI: 10.1111/bph.12167
PDE3, but not PDE4, reduces β₁ - and β₂-adrenoceptor-mediated inotropic and lusitropic effects in failing ventricle from metoprolol-treated patients
Abstract
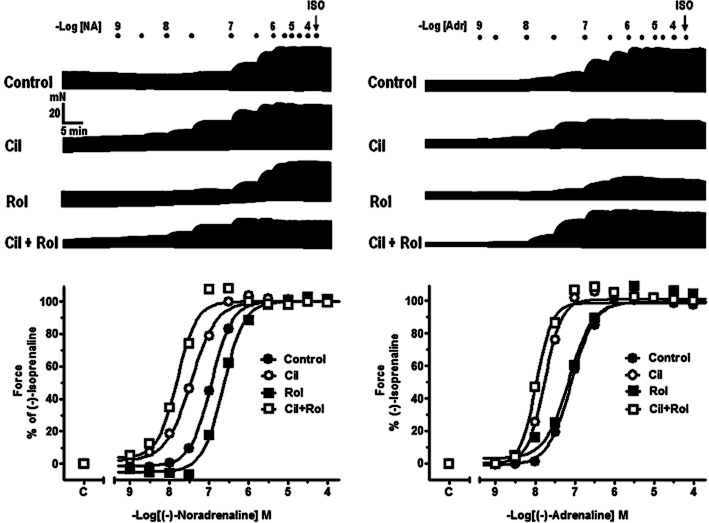
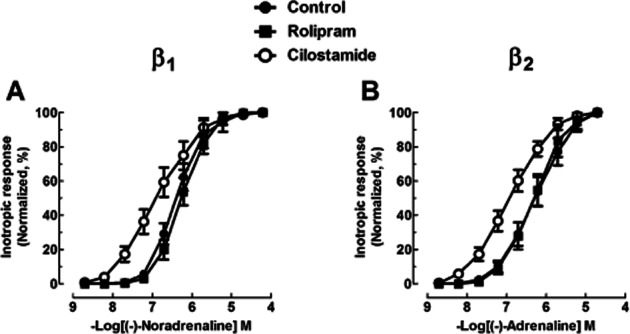
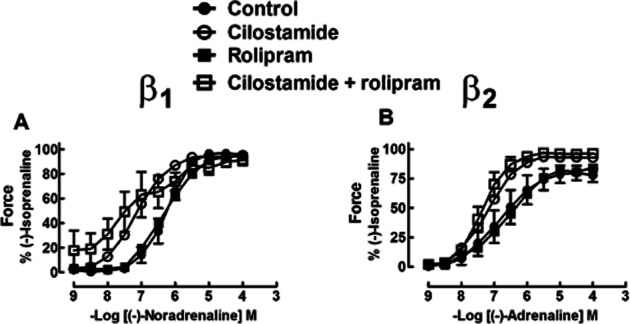
Background and purpose: PDE3 and/or PDE4 control ventricular effects of catecholamines in several species but their relative effects in failing human ventricle are unknown. We investigated whether the PDE3-selective inhibitor cilostamide (0.3-1 μM) or PDE4 inhibitor rolipram (1-10 μM) modified the positive inotropic and lusitropic effects of catecholamines in human failing myocardium.
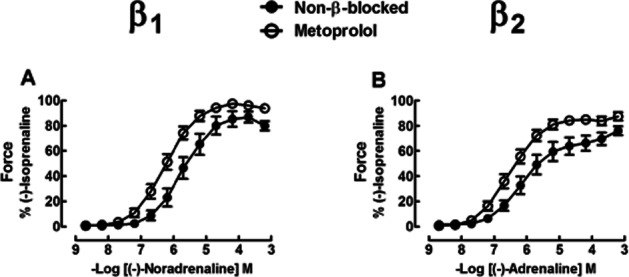
Experimental approach: Right and left ventricular trabeculae from freshly explanted hearts of 5 non-β-blocker-treated and 15 metoprolol-treated patients with terminal heart failure were paced to contract at 1 Hz. The effects of (-)-noradrenaline, mediated through β₁ adrenoceptors (β₂ adrenoceptors blocked with ICI118551), and (-)-adrenaline, mediated through β₂ adrenoceptors (β₁ adrenoceptors blocked with CGP20712A), were assessed in the absence and presence of PDE inhibitors. Catecholamine potencies were estimated from -logEC₅₀s.
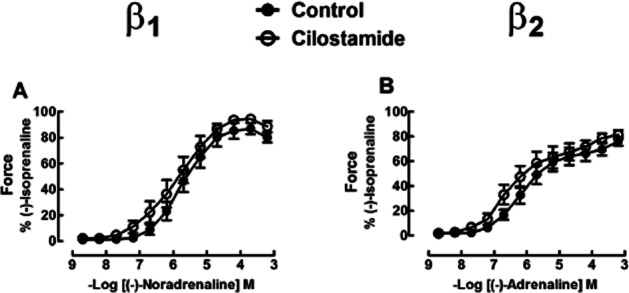
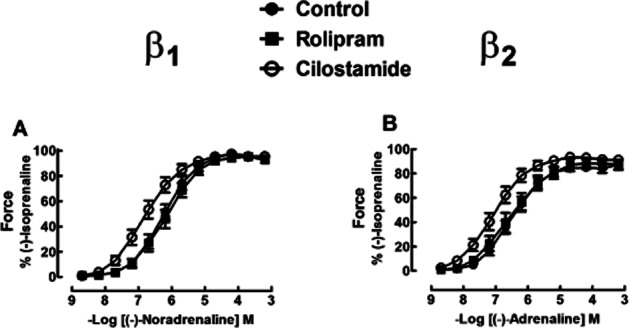
Key results: Cilostamide did not significantly potentiate the inotropic effects of the catecholamines in non-β-blocker-treated patients. Cilostamide caused greater potentiation (P = 0.037) of the positive inotropic effects of (-)-adrenaline (0.78 ± 0.12 log units) than (-)-noradrenaline (0.47 ± 0.12 log units) in metoprolol-treated patients. Lusitropic effects of the catecholamines were also potentiated by cilostamide. Rolipram did not affect the inotropic and lusitropic potencies of (-)-noradrenaline or (-)-adrenaline on right and left ventricular trabeculae from metoprolol-treated patients.
Conclusions and implications: Metoprolol induces a control by PDE3 of ventricular effects mediated through both β₁ and β₂ adrenoceptors, thereby further reducing sympathetic cardiostimulation in patients with terminal heart failure. Concurrent therapy with a PDE3 blocker and metoprolol could conceivably facilitate cardiostimulation evoked by adrenaline through β₂ adrenoceptors. PDE4 does not appear to reduce inotropic and lusitropic effects of catecholamines in failing human ventricle.
© 2013 The Authors. British Journal of Pharmacology © 2013 The British Pharmacological Society.
Figures
Comment in
-
PDE4 in the human heart - major player or little helper?Br J Pharmacol. 2013 Jun;169(3):524-7. doi: 10.1111/bph.12168. Br J Pharmacol. 2013. PMID: 23489196 Free PMC article.
References
-
- Bartel S, Stein B, Eschenhagen T, Mende U, Neumann J, Schmitz W, et al. Protein phosphorylation in isolated trabeculae from nonfailing and failing hearts. Mol Cell Biochem. 1996;157:171–179. - PubMed
-
- Bender AT, Beavo JA. Cyclic nucleotide phosphodiesterases: molecular regulation to clinical use. Pharmacol Rev. 2006;58:488–520. - PubMed
-
- Bootman MD, Smyrnias J, Thul R, Coombes S, Roderick HL. Atrial cardiomyocyte calcium signaling. Biochem Biophys Acta. 2011;1813:922–934. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
