

GFAP-BDP as an acute diagnostic marker in traumatic brain injury: results from the prospective transforming research and clinical knowledge in traumatic brain injury study
- PMID: 23489259
- PMCID: PMC3751263
- DOI: 10.1089/neu.2013.2883
GFAP-BDP as an acute diagnostic marker in traumatic brain injury: results from the prospective transforming research and clinical knowledge in traumatic brain injury study
Abstract
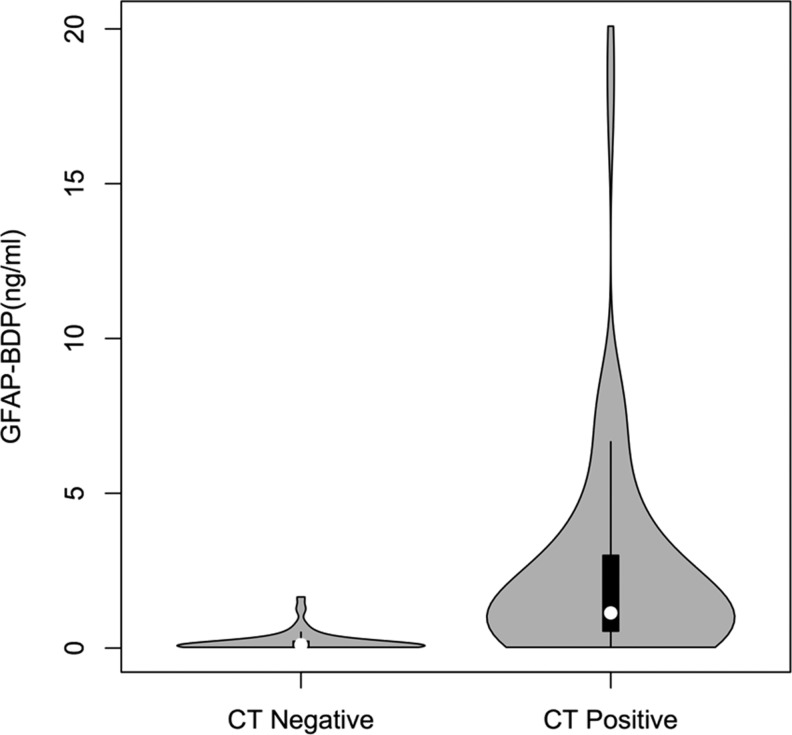
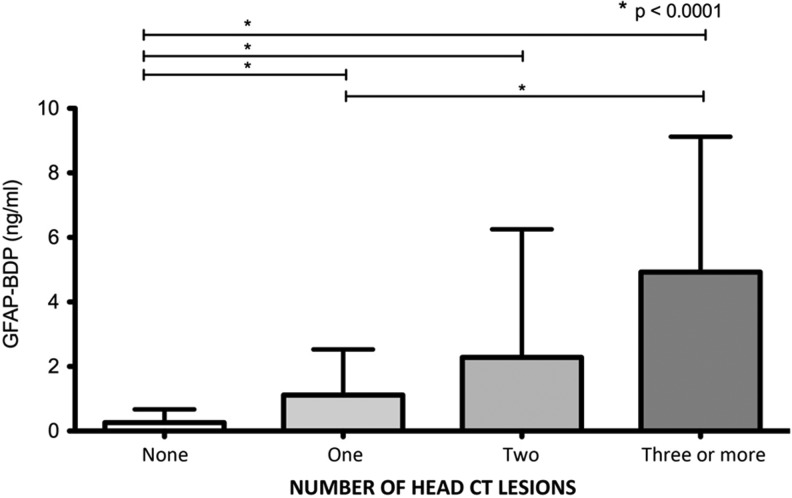
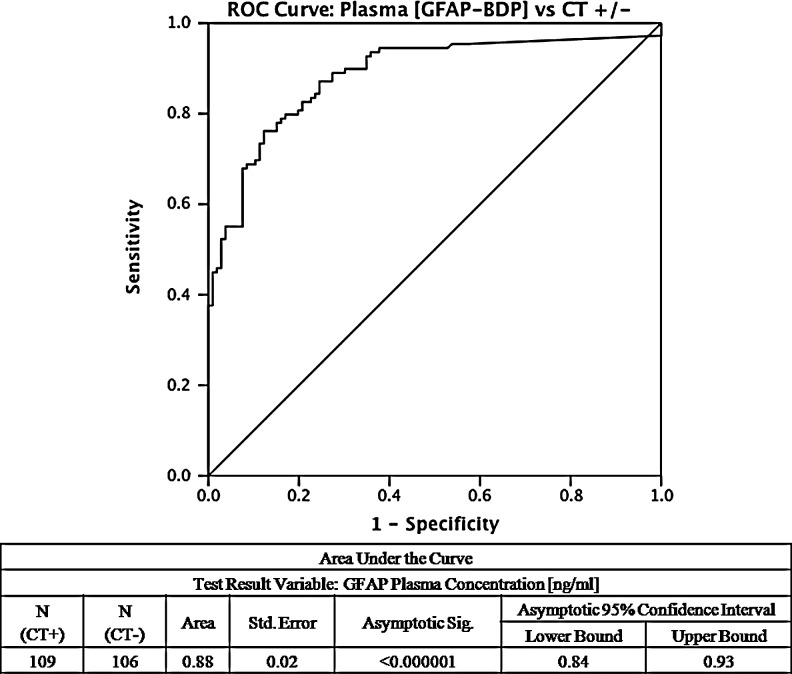
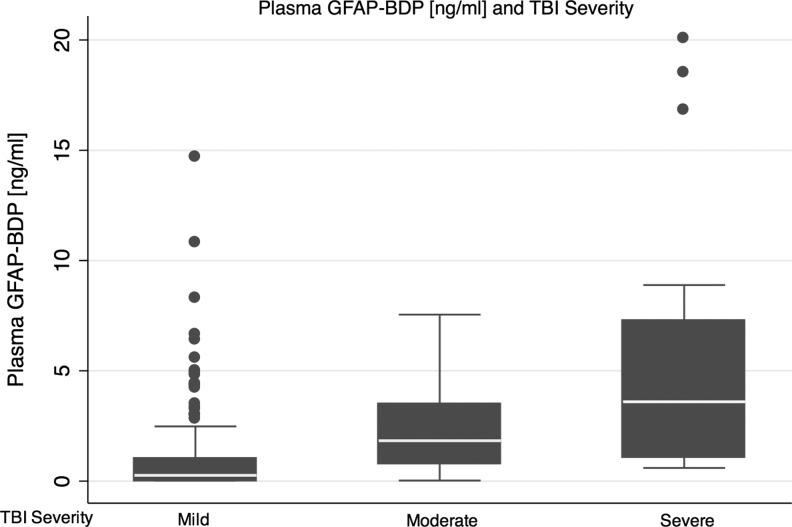
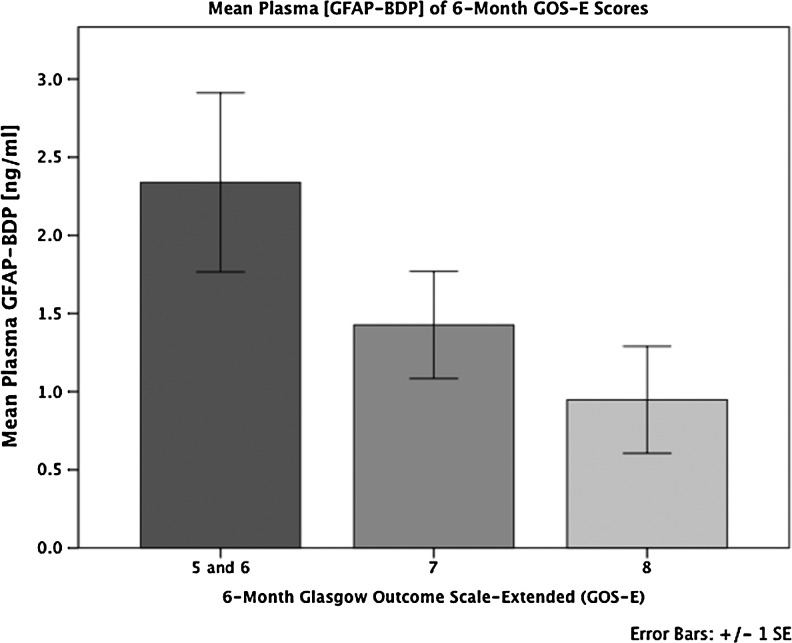
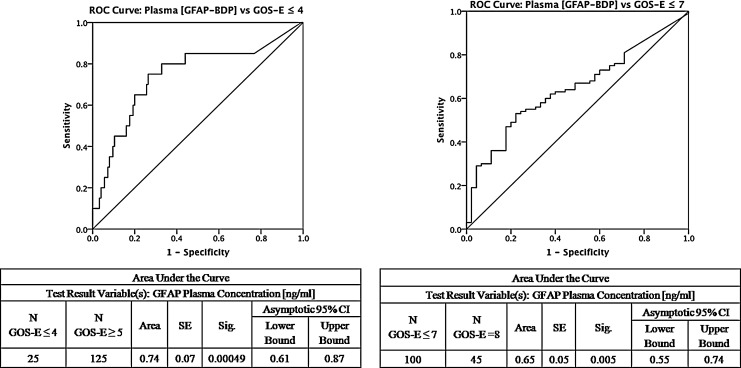
Reliable diagnosis of traumatic brain injury (TBI) is a major public health need. Glial fibrillary acidic protein (GFAP) is expressed in the central nervous system, and breakdown products (GFAP-BDP) are released following parenchymal brain injury. Here, we evaluate the diagnostic accuracy of elevated levels of plasma GFAP-BDP in TBI. Participants were identified as part of the prospective Transforming Research And Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Study. Acute plasma samples (<24 h post-injury) were collected from patients presenting with brain injury who had CT imaging. The ability of GFAP-BDP level to discriminate patients with demonstrable traumatic lesions on CT, and with failure to return to pre-injury baseline at 6 months, was evaluated by the area under the receiver operating characteristic curve (AUC). Of the 215 patients included for analysis, 83% had mild, 4% had moderate, and 13% had severe TBI; 54% had acute traumatic lesions on CT. The ability of GFAP-BDP level to discriminate patients with traumatic lesions on CT as evaluated by AUC was 0.88 (95% confidence interval [CI], 0.84-0.93). The optimal cutoff of 0.68 ng/mL for plasma GFAP-BDP level was associated with a 21.61 odds ratio for traumatic findings on head CT. Discriminatory ability of unfavorable 6 month outcome was lower, AUC 0.65 (95% CI, 0.55-0.74), with a 2.07 odds ratio. GFAP-BDP levels reliably distinguish the presence and severity of CT scan findings in TBI patients. Although these findings confirm and extend prior studies, a larger prospective trial is still needed to validate the use of GFAP-BDP as a routine diagnostic biomarker for patient care and clinical research. The term "mild" continues to be a misnomer for this patient population, and underscores the need for evolving classification strategies for TBI targeted therapy. (ClinicalTrials.gov number NCT01565551; NIH Grant 1RC2 NS069409).
Figures
References
-
- Vos P.E. Lamers K.J. Hendriks J.C. van Haaren M. Beems T. Zimmerman C. van Geel W. de Reus H. Biert J. Verbeek M.M. Glial and neuronal proteins in serum predict outcome after severe traumatic brain injury. Neurology. 2004;62:1303–1310. - PubMed
-
- Papa L. Lewis L.M. Silvestri S. Falk J.L. Giordano P. Brophy G.M. Demery J.A. Liu M.C. Mo J. Akinyi L. Mondello S. Schmid K. Robertson C.S. Tortella F.C. Hayes R.L. Wang K.K. J. Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention. Trauma Acute Care Surg. 2012;72:1335–1344. - PMC - PubMed
-
- Papa L. Lewis L.M. Falk J.L. Zhang Z. Silvestri S. Giordano P. Brophy G.M. Demery J.A. Dixit N.K. Ferguson I., et al. Elevated levels of serum glial fibrillary acidic protein breakdown products in mild and moderate traumatic brain injury are associated with intracranial lesions and neurosurgical intervention. Ann. Emerg. Med. 2012;59:471–483. - PMC - PubMed
-
- Yue J.K. Vassar M.J. Lingsma H. Cooper S.R. Yuh E.L. Mukherjee P. Puccio A.M. Gordon W. Okonkwo D.O. Valadka A. Schnyer D.M. Maas A. Manley G.T. Casey S.S. Cheong M. Dams-O'Connor K. Hricik A.J. Knight E.E. Kulubya E.S. Menon D. Morabito D.J. Pacheco J.L. Sinha T.K. Transforming research and clinical knowledge in traumatic brain injury (TRACK-TBI) pilot: Multicenter implementation of the common data elements for traumatic brain injury. J Neurotrauma. 2013 [Epub ahead of print] - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
