

Impact of cardiorespiratory fitness on the obesity paradox in patients with heart failure
- PMID: 23489451
- PMCID: PMC7242812
- DOI: 10.1016/j.mayocp.2012.11.020
Impact of cardiorespiratory fitness on the obesity paradox in patients with heart failure
Abstract
Objective: To determine the impact of cardiorespiratory fitness (FIT) on survival in relation to the obesity paradox in patients with systolic heart failure (HF).
Patients and methods: We studied 2066 patients with systolic HF (body mass index [BMI] ≥18.5 kg/m(2)) between April 1, 1993 and May 11, 2011 (with 1784 [86%] tested after January 31, 2000) from a multicenter cardiopulmonary exercise testing database who were followed for up to 5 years (mean ± SD, 25.0±17.5 months) to determine the impact of FIT (peak oxygen consumption <14 vs ≥14 mL O2 ∙ kg(-1) ∙ min(-1)) on the obesity paradox.
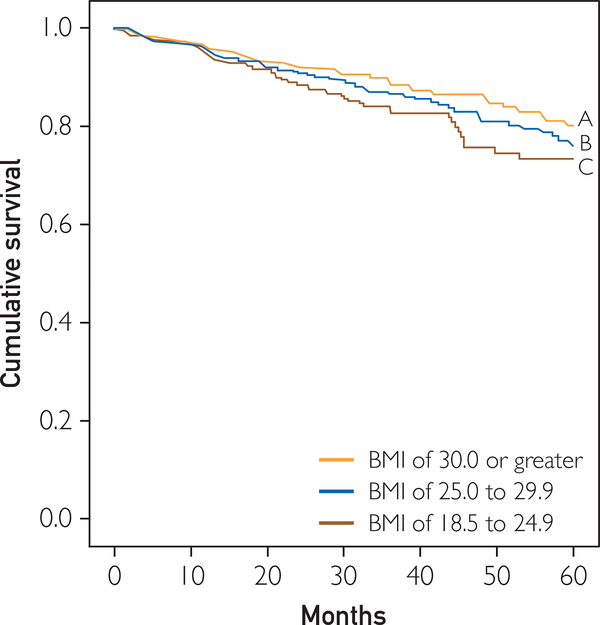
Results: There were 212 deaths during follow-up (annual mortality, 4.5%). In patients with low FIT, annual mortality was 8.2% compared with 2.8% in those with high FIT (P<.001). After adjusting for age and sex, BMI was a significant predictor of survival in the low FIT subgroup when expressed as a continuous (P=.03) and dichotomous (<25.0 vs ≥25.0 kg/m(2)) (P=.01) variable. Continuous and dichotomous BMI expressions were not significant predictors of survival in the overall and high FIT groups after adjusting for age and sex. In patients with low FIT, progressively worse survival was noted with BMI of 30.0 or greater, 25.0 to 29.9, and 18.5 to 24.9 (log-rank, 11.7; P=.003), whereas there was no obesity paradox noted in those with high FIT (log-rank, 1.72; P=.42).
Conclusion: These results indicate that FIT modifies the relationship between BMI and survival. Thus, assessing the obesity paradox in systolic HF may be misleading unless FIT is considered.
Copyright © 2013 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol. 2009;53(21):1925–1932. - PubMed
-
- Alpert MA. Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. Am J Med Sci. 2001; 321(14):225–236. - PubMed
-
- Lavie CJ, Milani RV, Ventura HO, Cardenas GA, Mehra MR, Messerli FH. Disparate effects of left ventricular geometry and obesity on mortality in patients with preserved left ventricular ejection fraction. Am J Cardiol. 2007;100(9):1460–1464. - PubMed
-
- Kenchaiah S, Evans JC, Levy D, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347(5):305–313. - PubMed
-
- Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Woo MA, Tillisch JH. The relationship between obesity and mortality in patients with heart failure. J Am Coll Cardiol. 2001; 38(3):789–795. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
