

Treating intractable phantom limb pain with ambulatory continuous peripheral nerve blocks: a pilot study
- PMID: 23489466
- PMCID: PMC3696484
- DOI: 10.1111/pme.12080
Treating intractable phantom limb pain with ambulatory continuous peripheral nerve blocks: a pilot study
Abstract
Background: There is currently no reliable treatment for phantom limb pain (PLP). Chronic PLP and associated cortical abnormalities may be maintained from abnormal peripheral input, raising the possibility that a continuous peripheral nerve block (CPNB) of extended duration may permanently reorganize cortical pain mapping, thus providing lasting relief.
Methods: Three men with below-the-knee (2) or -elbow (1) amputations and intractable PLP received femoral/sciatic or infraclavicular perineural catheter(s), respectively. Subjects were randomized in a double-masked fashion to receive perineural ropivacaine (0.5%) or normal saline for over 6 days as outpatients using portable electronic infusion pumps. Four months later, subjects returned for repeated perineural catheter insertion and received an ambulatory infusion with the alternate solution ("crossover"). Subjects were followed for up to 1 year.
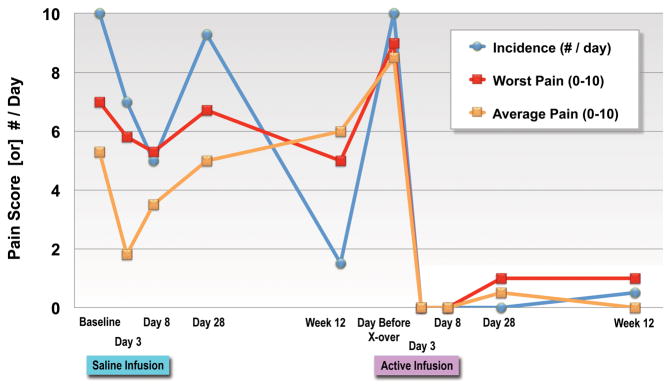
Results: By chance, all three subjects received saline during their initial infusion and reported little change in their PLP. One subject did not receive crossover treatment, but the remaining two subjects reported complete resolution of their PLP during and immediately following treatment with ropivacaine. One subject experienced no PLP recurrence through the 52-week follow-up period and the other reported mild PLP occurring once each week of just a small fraction of his original pain (pretreatment: continuous PLP rated 10/10; posttreatment: no PLP at baseline with average of one PLP episode each week rated 2/10) for 12 weeks (lost to follow-up thereafter).
Conclusions: A prolonged ambulatory CPNB may be a reliable treatment for intractable PLP. The results of this pilot study suggest that a large, randomized clinical trial is warranted.
Wiley Periodicals, Inc.
Conflict of interest statement
Figures
References
-
- Bloomquist T. Amputation and phantom limb pain: a pain-prevention model. AANA J. 2001;69:211–7. - PubMed
-
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89:422–9. - PubMed
-
- Nikolajsen L, Jensen TS. Phantom limb pain. Br J Anaesth. 2001;87:107–16. - PubMed
-
- Hazelgrove JF, Rogers PD. Phantom limb pain--a complication of lower extremity wound management. Int J Low Extrem Wounds. 2002;1:112–24. - PubMed
-
- Nikolajsen L, Ilkjaer S, Kroner K, Christensen JH, Jensen TS. The influence of preamputation pain on postamputation stump and phantom pain. Pain. 1997;72:393–405. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
