

Mitral apparatus assessment by delayed enhancement CMR: relative impact of infarct distribution on mitral regurgitation
- PMID: 23489536
- PMCID: PMC4048744
- DOI: 10.1016/j.jcmg.2012.08.016
Mitral apparatus assessment by delayed enhancement CMR: relative impact of infarct distribution on mitral regurgitation
Abstract
Objectives: This study sought to assess patterns and functional consequences of mitral apparatus infarction after acute myocardial infarction (AMI).
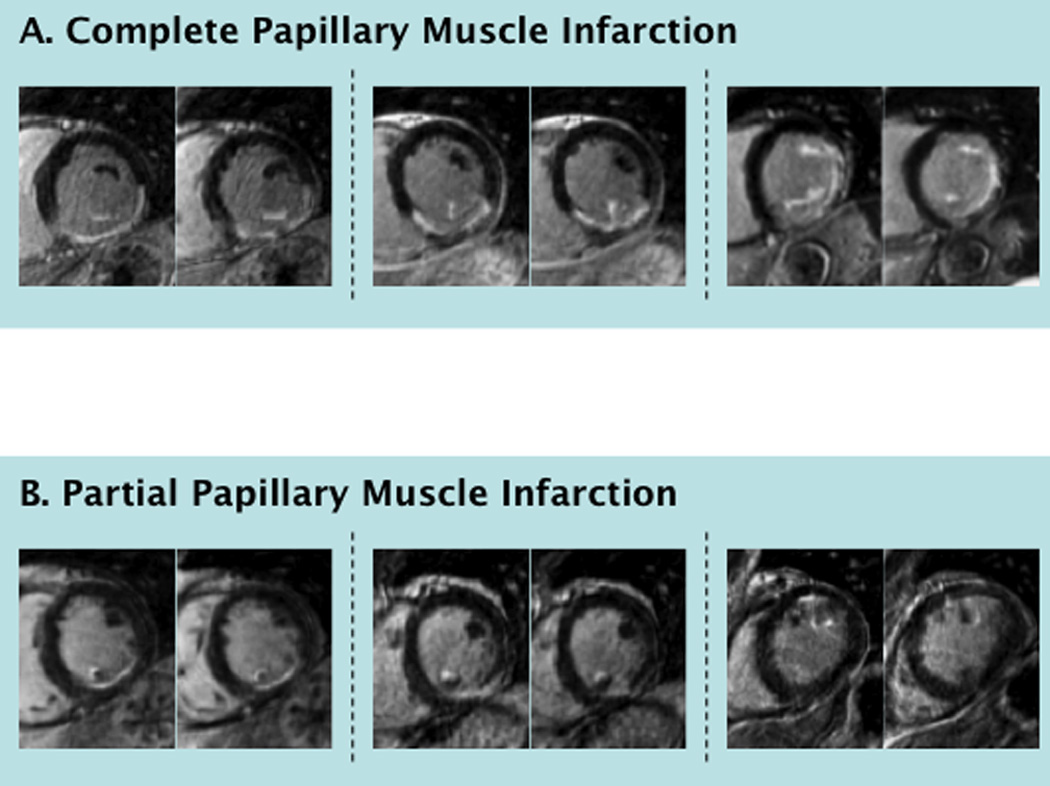
Background: The mitral apparatus contains 2 myocardial components: papillary muscles and the adjacent left ventricular (LV) wall. Delayed-enhancement cardiac magnetic resonance (DE-CMR) enables in vivo study of inter-relationships and potential contributions of LV wall and papillary muscle infarction (PMI) to mitral regurgitation (MR).
Methods: Multimodality imaging was performed: CMR was used to assess mitral geometry and infarct pattern, including 3D DE-CMR for PMI. Echocardiography was used to measure MR. Imaging occurred 27 ± 8 days after AMI (CMR, echocardiography within 1 day).
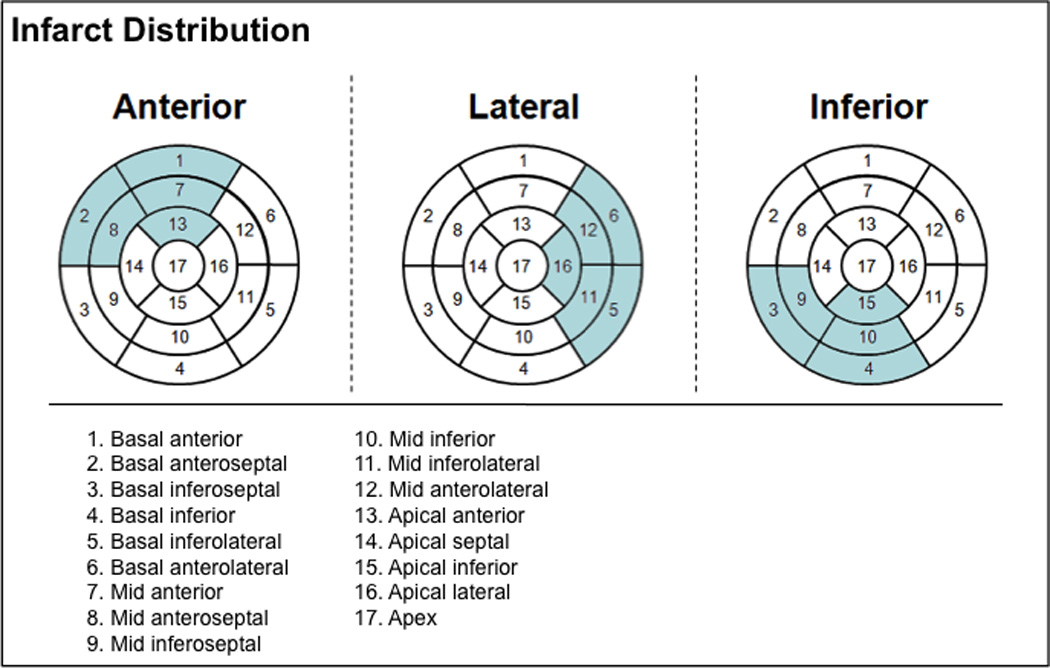
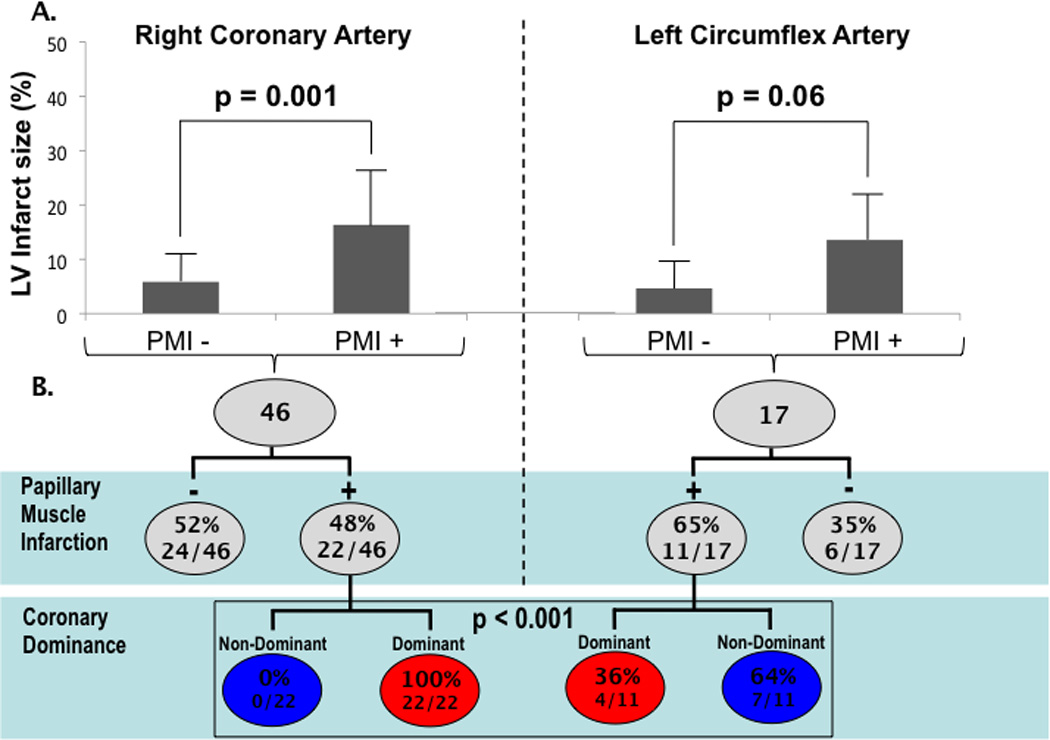
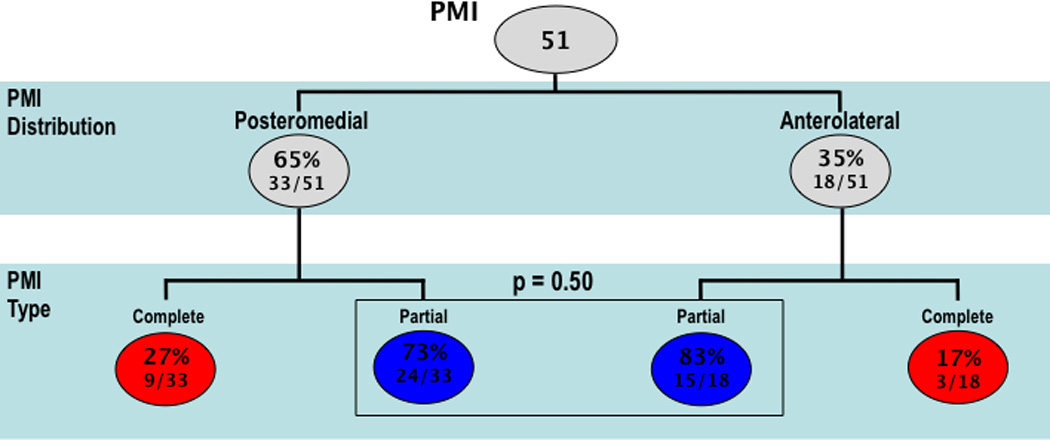
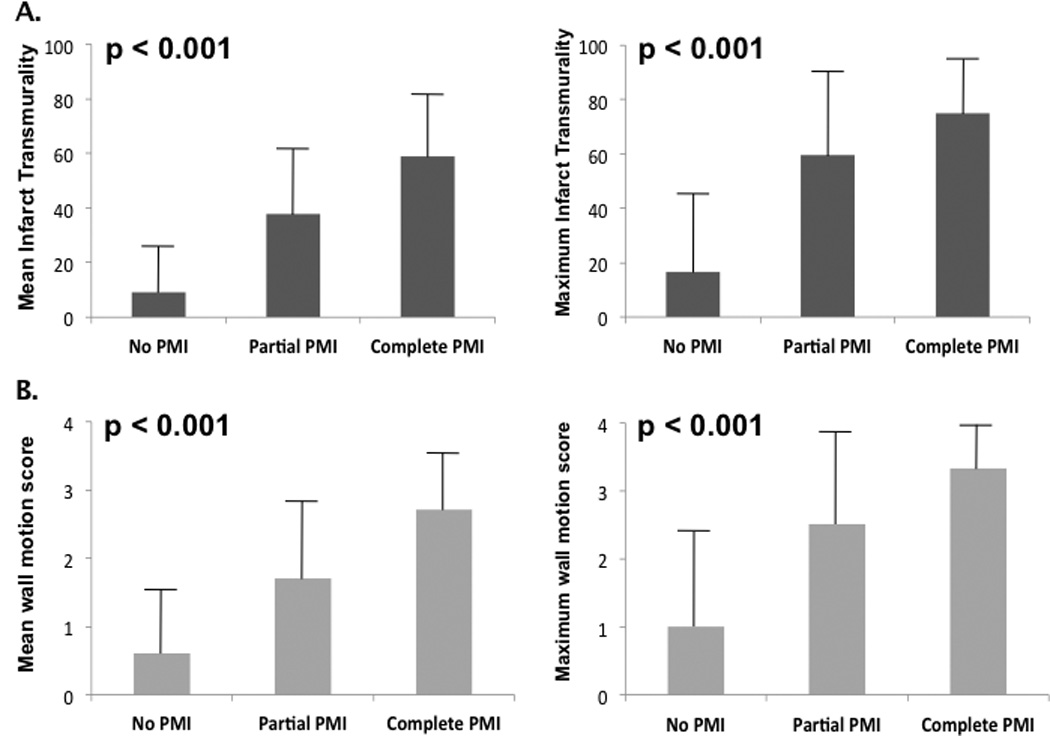
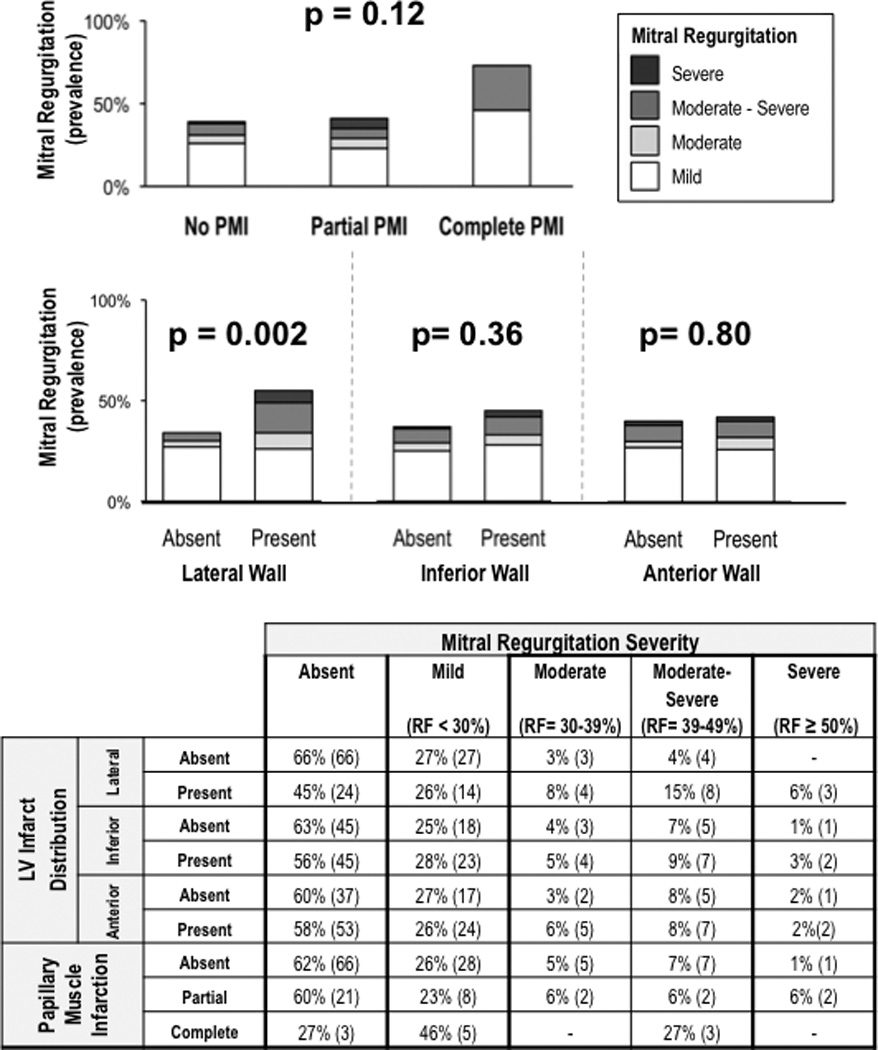
Results: A total of 153 patients with first AMI were studied; PMI was present in 30% (n = 46 [72% posteromedial, 39% anterolateral]). When stratified by angiographic culprit vessel, PMI occurred in 65% of patients with left circumflex, 48% with right coronary, and only 14% of patients with left anterior descending infarctions (p <0.001). Patients with PMI had more advanced remodeling as measured by LV size and mitral annular diameter (p <0.05). Increased extent of PMI was accompanied by a stepwise increase in mean infarct transmurality within regional LV segments underlying each papillary muscle (p <0.001). Prevalence of lateral wall infarction was 3-fold higher among patients with PMI compared to patients without PMI (65% vs. 22%, p <0.001). Infarct distribution also impacted MR, with greater MR among patients with lateral wall infarction (p = 0.002). Conversely, MR severity did not differ on the basis of presence (p = 0.19) or extent (p = 0.12) of PMI, or by angiographic culprit vessel. In multivariable analysis, lateral wall infarct size (odds ratio 1.20/% LV myocardium [95% confidence interval: 1.05 to 1.39], p = 0.01) was independently associated with substantial (moderate or greater) MR even after controlling for mitral annular (odds ratio 1.22/mm [1.04 to 1.43], p = 0.01), and LV end-diastolic diameter (odds ratio 1.11/mm [0.99 to 1.23], p = 0.056).
Conclusions: Papillary muscle infarction is common after AMI, affecting nearly one-third of patients. Extent of PMI parallels adjacent LV wall injury, with lateral infarction-rather than PMI-associated with increased severity of post-AMI MR.
Trial registration: ClinicalTrials.gov NCT00539045.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Ischemic mitral regurgitation: in search of the culprit.JACC Cardiovasc Imaging. 2013 Feb;6(2):235-7. doi: 10.1016/j.jcmg.2012.11.006. JACC Cardiovasc Imaging. 2013. PMID: 23489537 No abstract available.
References
-
- Amigoni M, Meris A, Thune JJ, Mangalat D, Skali H, Bourgoun M, Warnica JW, Barvik S, Arnold JM, Velazquez EJ, Van de Werf F, Ghali J, McMurray JJ, Kober L, Pfeffer MA, Solomon SD. Mitral regurgitation in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both: prognostic significance and relation to ventricular size and function. Eur Heart J. 2007;28(3):326–333. - PubMed
-
- Lamas GA, Mitchell GF, Flaker GC, Smith SC, Jr, Gersh BJ, Basta L, Moye L, Braunwald E, Pfeffer MA. Clinical significance of mitral regurgitation after acute myocardial infarction. Survival and Ventricular Enlargement Investigators. Circulation. 1997;96(3):827–833. - PubMed
-
- Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation. 2001;103(13):1759–1764. - PubMed
-
- Ennezat PV, Darchis J, Lamblin N, Tricot O, Elkohen M, Aumegeat V, Equine O, Dujardin X, Saadouni H, Le Tourneau T, de Groote P, Bauters C. Left ventricular remodeling is associated with the severity of mitral regurgitation after inaugural anterior myocardial infarction--optimal timing for echocardiographic imaging. Am Heart J. 2008;155(5):959–965. - PubMed
-
- Neskovic AN, Marinkovic J, Bojic M, Popovic AD. Early predictors of mitral regurgitation after acute myocardial infarction. Am J Cardiol. 1999;84(3):329–332. A328. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
