

Digoxin reduces 30-day all-cause hospital admission in older patients with chronic systolic heart failure
- PMID: 23490060
- PMCID: PMC3926199
- DOI: 10.1016/j.amjmed.2013.02.001
Digoxin reduces 30-day all-cause hospital admission in older patients with chronic systolic heart failure
Abstract
Background: Heart failure is a leading cause of hospital admission and readmission in older adults. The new United States healthcare reform law has created provisions for financial penalties for hospitals with higher than expected 30-day all-cause readmission rates for hospitalized Medicare beneficiaries aged ≥65 years with heart failure. We examined the effect of digoxin on 30-day all-cause hospital admission in older patients with heart failure and reduced ejection fraction.
Methods: In the main Digitalis Investigation Group trial, 6800 ambulatory patients with chronic heart failure (ejection fraction ≤45%) were randomly assigned to digoxin or placebo. Of these, 3405 were aged ≥65 years (mean age, 72 years; 25% were women; 11% were nonwhite). The main outcome in the current analysis was 30-day all-cause hospital admission.
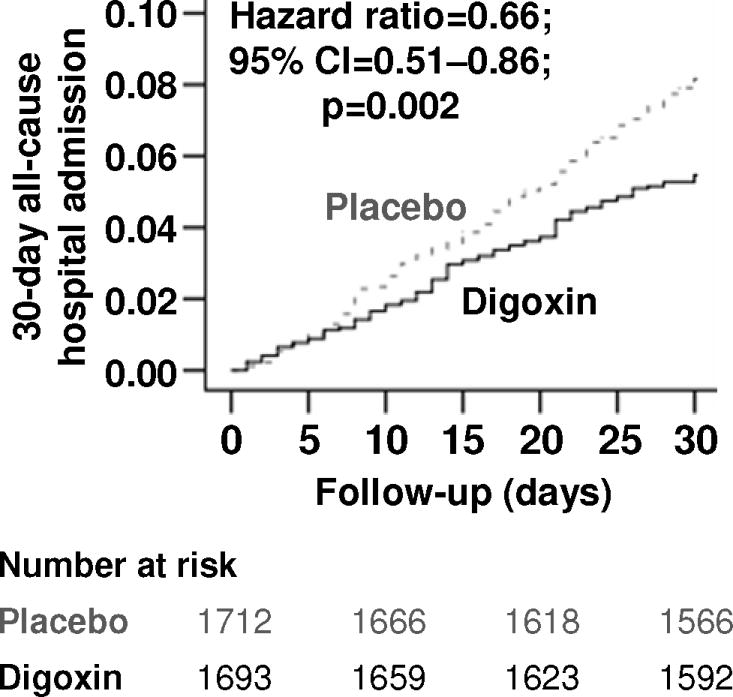
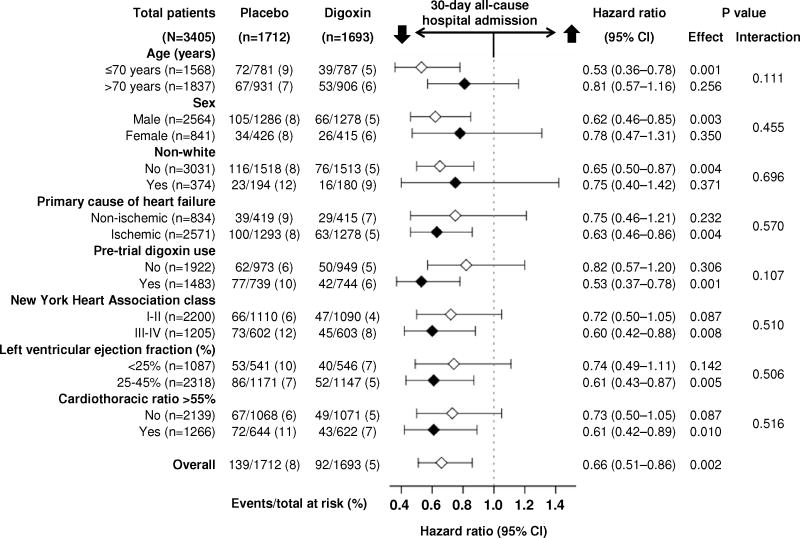
Results: In the first 30 days after randomization, all-cause hospitalization occurred in 5.4% (92/1693) and 8.1% (139/1712) of patients in the digoxin and placebo groups, respectively, (hazard ratio {HR} when digoxin was compared with placebo, 0.66; 95% confidence interval {CI}, 0.51-0.86; P=.002). Digoxin also reduced both 30-day cardiovascular (3.5% vs 6.5%; HR, 0.53; 95% CI, 0.38-0.72; P<.001) and heart failure (1.7 vs 4.2%; HR, 0.40; 95% CI, 0.26-0.62; P<.001) hospitalizations, with similar trends for 30-day all-cause mortality (0.7% vs 1.3%; HR, 0.55; 95% CI, 0.27-1.11; P=.096). Younger patients were at lower risk of events but obtained similar benefits from digoxin.
Conclusions: Digoxin reduces 30-day all-cause hospital admission in ambulatory older patients with chronic systolic heart failure. Future studies need to examine its effect on 30-day all-cause hospital readmission in hospitalized patients with acute heart failure.
Keywords: 30-day all-cause hospital admission; Digoxin; Heart failure.
Published by Elsevier Inc.
Figures
Comment in
-
The reply.Am J Med. 2014 Mar;127(3):e13. doi: 10.1016/j.amjmed.2013.11.007. Epub 2013 Dec 8. Am J Med. 2014. PMID: 24321411 No abstract available.
-
The endless story of digitalis.Am J Med. 2014 Mar;127(3):e11. doi: 10.1016/j.amjmed.2013.08.026. Am J Med. 2014. PMID: 24560326 No abstract available.
-
Use of digoxin in chronic systolic heart failure in current era.Am J Med. 2015 Jan;128(1):e17. doi: 10.1016/j.amjmed.2014.03.030. Am J Med. 2015. PMID: 25553632 No abstract available.
-
The reply.Am J Med. 2015 Jan;128(1):e19. doi: 10.1016/j.amjmed.2014.09.014. Am J Med. 2015. PMID: 25553633 No abstract available.
References
-
- Jiang HJ, Russo CA, Barrett ML. HCUP Statistical Brief #72. U S Agency for Healthcare Research and Quality; Rockville, MD: Apr, 2009. Nationwide Frequency and Costs of Potentially Preventable Hospitalizations, 2006. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb72.pdf. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. The New England journal of medicine. 2009;360:1418–1428. - PubMed
-
- Stone J, Hoffman GJ. Congressional Research Service Report for Congress. Prepared for Members and Committees of Congress; Washington, DC: 2010. Medicare Hospital Readmissions: Issues, Policy Options and PPACA.
-
- The Centers for Medicare & Medicaid Services. [December 28, 2012];Readmissions Reduction Program. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpati....
-
- Rau J. Hospitals Face Pressure to Avert Readmissions. [December 2, 2012];The New York Times. http://www.nytimes.com/2012/11/27/health/hospitals-face-pressure-from-me..., Published:November 26, 2012;Health.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
