

Surgical treatment of lateral clavicle fractures associated with complete coracoclavicular ligament disruption: Clinico-radiological outcomes of acromioclavicular joint sparing and spanning implants
- PMID: 23493665
- PMCID: PMC3590702
- DOI: 10.4103/0973-6042.106224
Surgical treatment of lateral clavicle fractures associated with complete coracoclavicular ligament disruption: Clinico-radiological outcomes of acromioclavicular joint sparing and spanning implants
Abstract
Purpose: Distal clavicle fracture associated with complete coracoclavicular ligament disruption represents an unstable injury, and osteosynthesis is recommended. This study was performed (1) to retrospectively analyse the clinico-radiological outcomes of two internal fixation techniques, and (2) to identify and analyse radiographic fracture patterns of fracture that are associated with this injury.
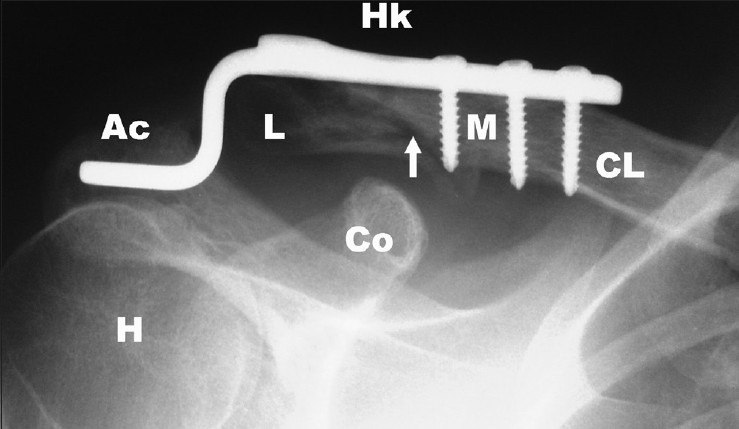
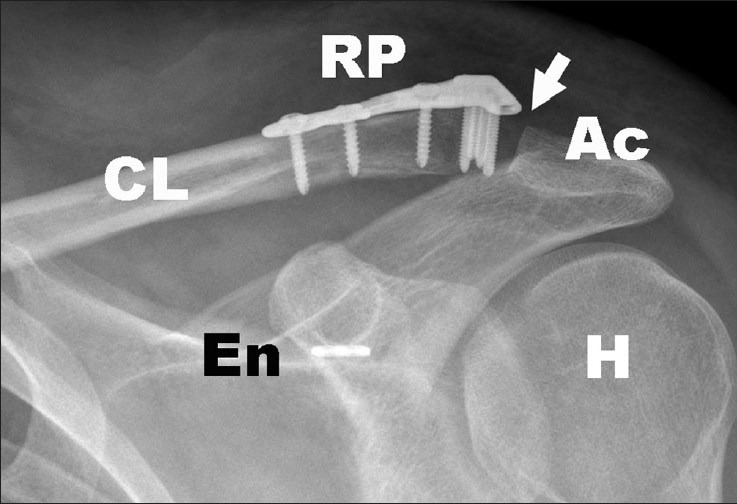
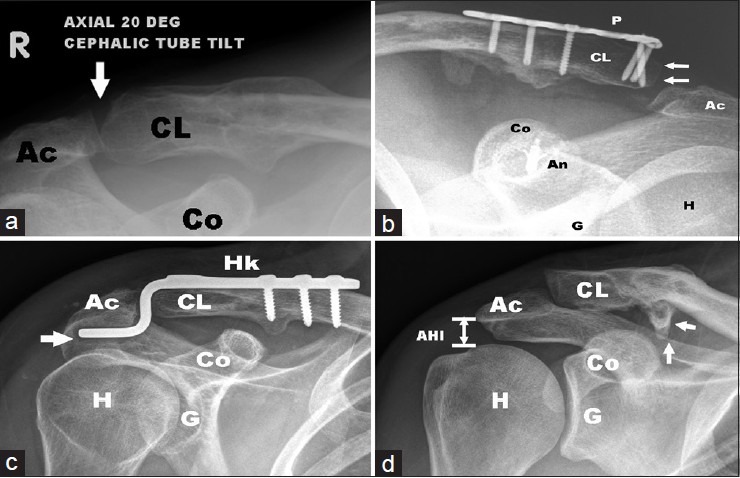
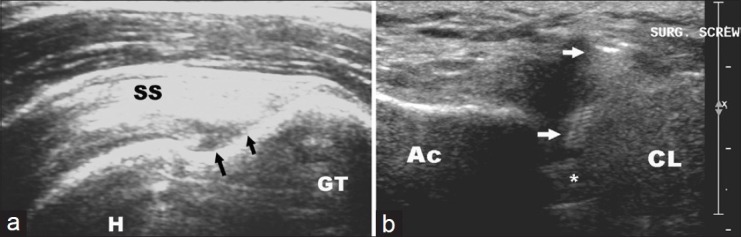
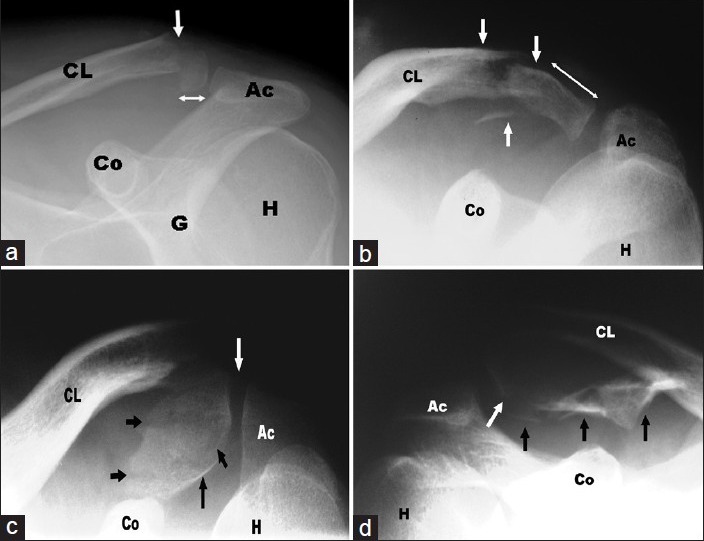
Materials and methods: A total of 15 patients underwent osteosynthesis with either (1) acromioclavicular joint-spanning implants (Group 1, Hook plate device, n = 10) or (2) joint-sparing implants (Group 2, distal radius plate, n = 5); these were reviewed at a mean period of 26.1 months (12 to 40 months). Clinical outcomes were measured using Constant Score (CS), Simple Shoulder Test (SST), and Walch ACJ score (WS). Radiographs and ultrasonography were used to assess the glenohumeral and acromioclavicular joints, and the subacromial space. Preoperative radiographs were analyzed for assessment of fracture lines to identify radiographic patterns. Statistical analysis of the data was performed to determine any significant differences between the two groups.
Results: The overall clinical outcome was satisfactory (CS 80.8, SST 11.3, WS 17.6) and a high union rate (93.3%) was observed. Radiographic complications (acromioclavicular degeneration and subluxation, hook migration, abnormal ossification) did not negatively influence the final clinical outcomes. Four distinct radiographic fracture patterns were observed. A statistically significant difference ( P < 0.05) was observed in the reoperation rates between the two groups.
Conclusions: Internal fixation of this fracture pattern is associated with a high union rate and favorable clinical outcomes with both techniques. A combination of distal radius plate and ligament reconstruction device resulted in stable fixation and significantly lower reoperation rates, and should be used when fracture geometry permits (Types 1 and 2).
Design: Retrospective review of a consecutive clinical case series.
Setting: Level 1 academic trauma service, Public Hospital.
Keywords: Acromioclavicular joint; comminution; distal clavicle fracture; fracture patterns; hook plate; locking radius plate; ultrasound.
Conflict of interest statement
Figures
References
-
- Edwards DJ, Kavanagh TG, Flannery MC. Fractures of the distal clavicle: A case for fixation. Injury. 1992;23:44–6. - PubMed
-
- Neer CS., 2nd Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma. 1963;3:99–110. - PubMed
-
- Rokito AS, Zuckerman JD, Shaari JM, Eisenberg DP, Cuomo F, Gallagher MA. A comparison of nonoperative and operative treatment of type II distal clavicle fractures. Bull Hosp Jt Dis. 2002-2003;61:32–9. - PubMed
-
- Chandrasen J, Badhe S, Cresswell T, De Beer J. The clavicular hook plate: Consequences in three cases. Eur J Trauma Emerg Surg. 2007;33:557–9. - PubMed
-
- Charity RM, Haidar SG, Ghosh S, Tillu AB. Fixation failure of the clavicular hook plate: A report of three cases. J Orthop Surg (Hong Kong) 2006;14:333–5. - PubMed
LinkOut - more resources
Full Text Sources
