

Laminarthrectomy as a surgical approach for decompressing the spinal canal: assessment of preoperative versus postoperative dural sac cross-sectional areal (DSCSA)
- PMID: 23494757
- PMCID: PMC3731479
- DOI: 10.1007/s00586-013-2737-1
Laminarthrectomy as a surgical approach for decompressing the spinal canal: assessment of preoperative versus postoperative dural sac cross-sectional areal (DSCSA)
Abstract
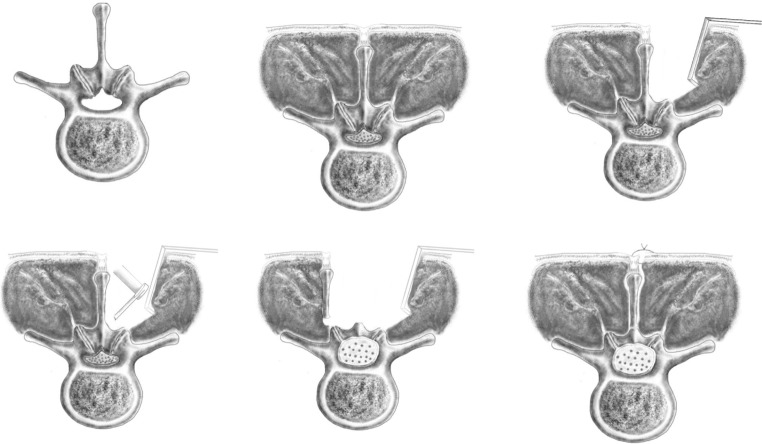
Introduction: Surgery for lumbar spinal stenosis (LSS) is today the most frequently performed procedure in the adult lumbar spine. Long-term benefit of surgery for LSS is well documented both in randomized and in non-randomized trials. In this paper, we present the results from laminarthrectomy as an alternative surgical approach, which have theoretical advantages over other approaches. In this study, we wanted to study the clinical and radiological results of laminarthrectomy. Dural sac cross-sectional areal (DSCSA) is an objective method to quantify the degree of central stenosis in the spinal canal, and was used to measure whether we were able to achieve an adequate decompression of the spinal canal with laminarthrectomy as a surgical approach.
Materials and methods: All patients operated on with this approach consecutively in the period 1 January 2008 to 31 March 2009 were included in the study. All perioperative complications were noted. Clinical results were measured by means of a questionnaire. The patients that agreed to attend the study had an MRI taken of the operated level. DSCSA before and after surgery of the actual level were measured by three observers. We then performed a correlation test between increase of area and clinical results. We also tested for inter- and intra-observer reability.
Results: Fifty-six laminarthrectomy were performed. There were 17% complications, none of them were life-threatening or disabling. 46 patients attended the study and answered the questionnaire. Thirty-four patients (83%) reported clinical improvement, whereas six (13%) patients reported no improvement, and two (4%) patients reported that they were worse. Mean ODI was 23.0. Mean EQ-5D was 0.77. Mean VAS-score for back-pain was 3.1 and mean VAS-score for leg-pain was 2.8. Mean DSCSA were measured to 80 mm(2) before surgery and 161 mm(2) after surgery. That gave an increase of DSCSA of 81 mm(2) (101%). We found a significant positive correlation between increase of area and clinical results. We also found consistent inter- and intra-observer reability.
Discussion: In this study, the clinical results of laminarthrectomy were good, and comparable with other reports for LSS. The rates of complications are also comparable with other reports in spinal surgery. A significant increase in the spinal canal diameter was achieved. Within the limitations a retrospective study gives, we conclude that laminarthrectomy seems to be a safe and effective surgical approach for significant decompressing the adult central spinal canal, and measurement of DSCSA, before and after surgery seems to be a good way to quantify the degree of decompression.
Figures



References
-
- Ciol MA, Deyo RA, Howell E, Kreif S. An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr Soc. 1996;44:285–290. - PubMed
-
- Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleas F (2000) Lumbar spinal stenosis: conservative or surgical management? A prospective 10-year study. Spine (Phila Pa 1976) 25:1424–1435 - PubMed
-
- Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976) 30:936–943 - PubMed
-
- Gibson JN, Waddell G (2005) Surgery for degenerative lumbar spondylosis: updated Cochrane review. Spine (Phila Pa 1976) 30:2312–2320 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
