

Improved intensive care unit survival for critically ill allogeneic haematopoietic stem cell transplant recipients following reduced intensity conditioning
- PMID: 23496350
- PMCID: PMC4296346
- DOI: 10.1111/bjh.12294
Improved intensive care unit survival for critically ill allogeneic haematopoietic stem cell transplant recipients following reduced intensity conditioning
Abstract
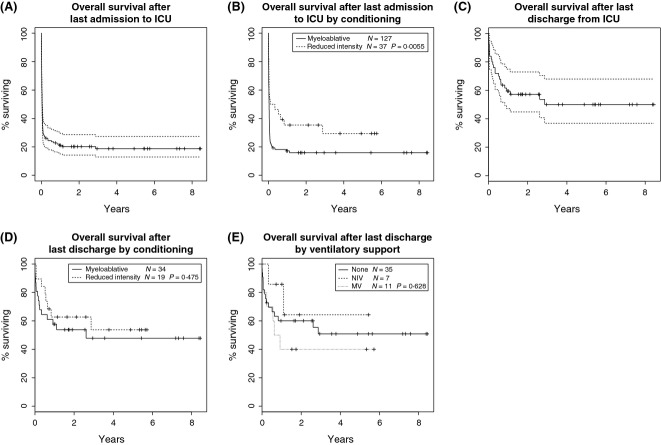
The use of allogeneic haematopoietic stem cell transplantation (Allo-HSCT) is a standard treatment option for many patients with haematological malignancies. Historically, patients requiring intensive care unit (ICU) admission for transplant-related toxicities have fared extremely poorly, with high ICU mortality rates. Little is known about the impact of reduced intensity Allo-HSCT conditioning regimens in older patients on the ICU and subsequent long-term outcomes. A retrospective analysis of data collected from 164 consecutive Allo-HSCT recipients admitted to ICU for a total of 213 admissions, at a single centre over an 11·5-year study period was performed. Follow-up was recorded until 31 March 2011. Autologous HSCT recipients were excluded. In this study we report favourable ICU survival following Allo-HSCT and, for the first time, demonstrate significantly better survival for patients who underwent Allo-HSCT with reduced intensity conditioning compared to those treated with myeloablative conditioning regimens. In addition, we identified the need for ventilation (invasive or non-invasive) as an independently significant adverse factor affecting short-term ICU outcome. For patients surviving ICU admission, subsequent long-term overall survival was excellent; 61% and 51% at 1 and 5 years, respectively. Reduced intensity Allo-HSCT patients admitted to ICU with critical illness have improved survival compared to myeloablative Allo-HSCT recipients.
© 2013 John Wiley & Sons Ltd.
Figures
References
-
- Afessa B, Tefferi A, Hoagland HC, Letendre L, Peters SG. Outcome of recipients of bone marrow transplants who require intensive-care unit support. Mayo Clinic Proceedings. 1992;67:117–122. - PubMed
-
- Afessa B, Tefferi A, Dunn WF, Litzow MR, Peters SG. Intensive care unit support and acute physiology and chronic health evaluation III performance in hematopoietic stem cell transplant recipients. Critical Care Medicine. 2003;31:1715–1721. - PubMed
-
- Azoulay E, Pochard F, Chevret S, Vinsonneau C, Garrouste M, Cohen Y, Thuong M, Paugam C, Apperre C, De Cagny B, Brun F, Bornstain C, Parrot A, Thamion F, Lacherade JC, Bouffard Y, Le Gall JR, Herve C, Grassin M, Zittoun R, Schlemmer B, Dhainaut JF. Compliance with triage to intensive care recommendations. Critical Care Medicine. 2001;29:2132–2136. - PubMed
-
- Bach PB, Schrag D, Nierman DM, Horak D, White P, Jr, Young JW, Groeger JS. Identification of poor prognostic features among patients requiring mechanical ventilation after hematopoietic stem cell transplantation. Blood. 2001;98:3234–3240. - PubMed
-
- Bacigalupo A, Sormani MP, Lamparelli T, Gualandi F, Occhini D, Bregante S, Raiola AM, di Grazia C, Dominietto A, Tedone E, Piaggio G, Podesta M, Bruno B, Oneto R, Lombardi A, Frassoni F, Rolla D, Rollandi G, Viscoli C, Ferro C, Garbarino L, Van Lint MT. Reducing transplant-related mortality after allogeneic hematopoietic stem cell transplantation. Haematologica. 2004;89:1238–1247. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
