

Corticosteroid therapy in a patient with cerebral amyloid angiopathy-related inflammation
- PMID: 23497126
- PMCID: PMC3635896
- DOI: 10.1186/1742-2094-10-39
Corticosteroid therapy in a patient with cerebral amyloid angiopathy-related inflammation
Abstract
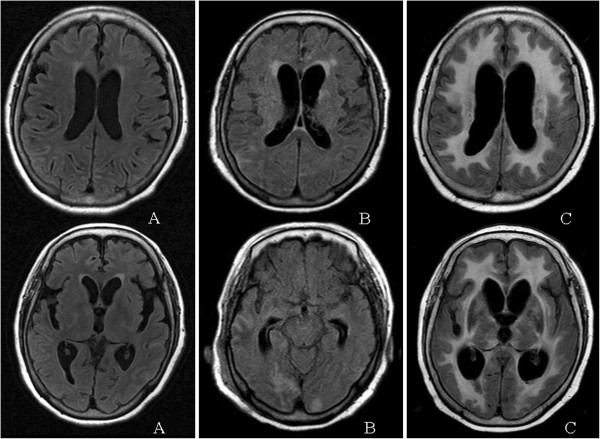
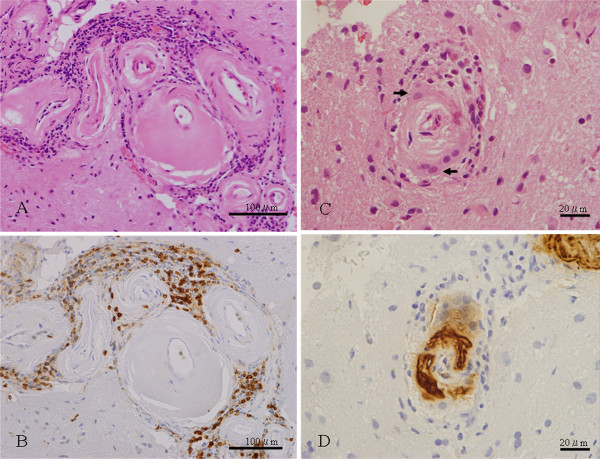
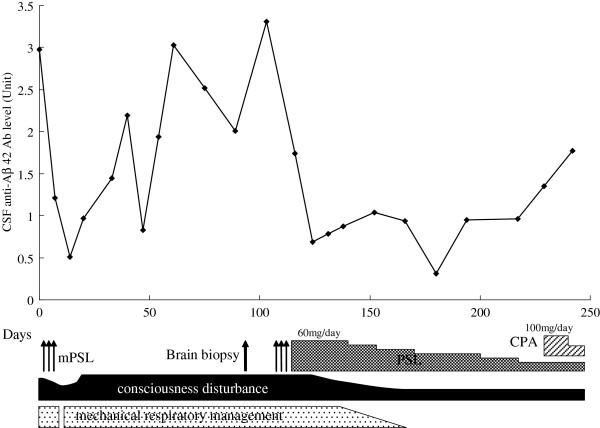
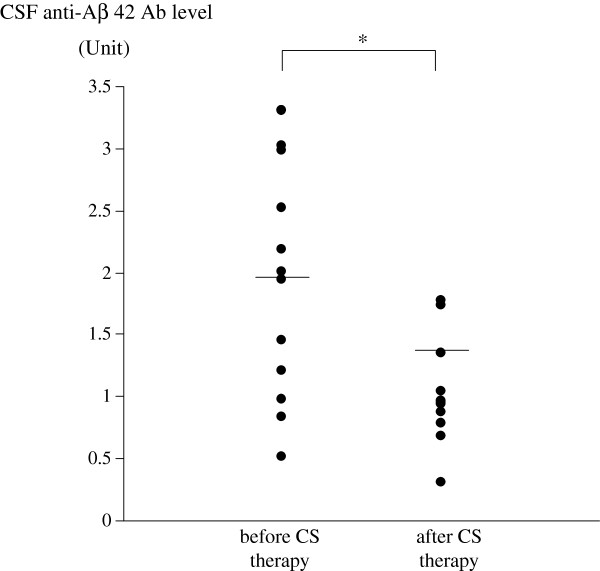
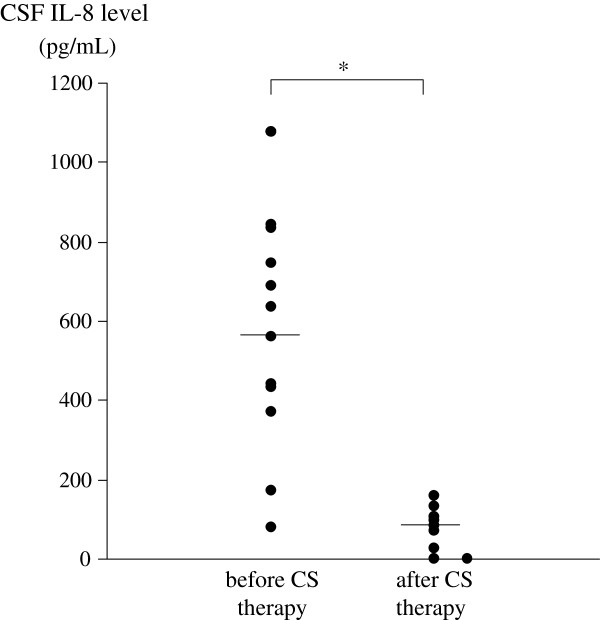
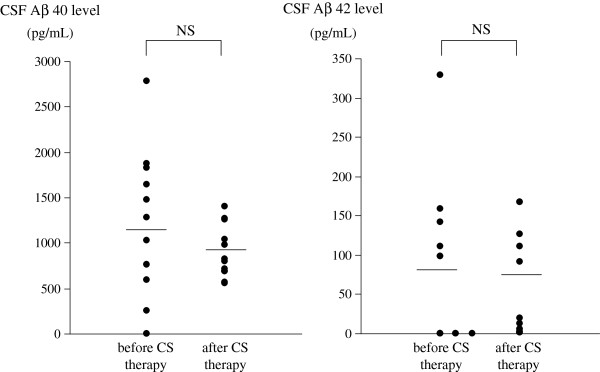
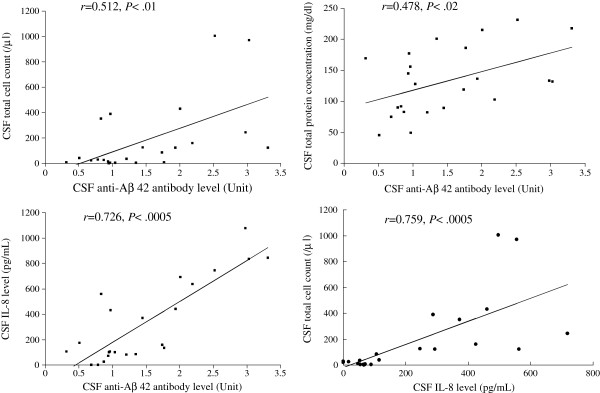
We studied longitudinal changes of the levels of anti-amyloid β (anti-Aβ) antibody, amyloid β (Aβ) protein, and interleukin 8 (IL-8) in cerebrospinal fluid (CSF) of a patient with cerebral amyloid angiopathy-related inflammation (CAA-ri) in whom steroid treatment resulted in clinical improvement. The diagnosis of CAA-ri was established with brain biopsy. Levels of anti-Aβ 42 antibody, Aβ 40, Aβ 42 and IL-8 in CSF were measured in the CAA-ri patient at 23 time points in the 8-month clinical course. These CSF samples were divided into 2 groups: those obtained before (n = 12) and those after (n = 11) oral corticosteroid therapy was started. We compared these levels between CSF samples obtained before and after therapy. The mean levels of anti-Aβ 42 antibody and IL-8 were significantly higher in CSF samples of the CAA-ri patient before oral corticosteroid therapy than those after therapy. A positive correlation was noted between levels of anti-Aβ 42 antibodies and IL-8 in CSF of this patient. There were no significant differences of mean levels of Aβ 40 and Aβ 42 between CSF samples obtained before and after oral corticosteroid therapy. It was possible that the autoinflammatory process with anti-Aβ 42 antibodies and IL-8 may have been involved in the pathogenesis of CAA-ri, and that corticosteroid therapy directly affected levels of anti-Aβ 42 antibody and IL-8. In summary, CAA-ri encephalopathy is a relapsing or progressive disorder and may be treatable by adequate immunosuppressive therapy. The anti-Aβ 42 antibody in CSF is a useful biological marker for therapeutic monitoring of CAA-ri.
Figures
References
-
- Scolding NJ, Joseph F, Kirby PA, Mazanti I, Gray F, Mikol J, Ellison D, Hilton DA, Williams TL, MacKenzie JM, Xuereb JH, Love S. Abeta-related angiitis: primary angiitis of the central nervous system associated with cerebral amyloid angiopathy. Brain. 2005;128:500–515. doi: 10.1093/brain/awh379. - DOI - PubMed
-
- Sakaguchi H, Ueda A, Kosaka T, Yamashita S, Kimura E, Yamashita T, Maeda Y, Hirano T, Uchino M. Cerebral amyloid angiopathy-related inflammation presenting with steroid-responsive higher brain dysfunction: case report and review of the literature. J Neuroinflammation. 2011;8:116. doi: 10.1186/1742-2094-8-116. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
