

Induction chemotherapy in patients with resectable head and neck squamous cell carcinoma: a meta-analysis
- PMID: 23497185
- PMCID: PMC3601969
- DOI: 10.1186/1477-7819-11-67
Induction chemotherapy in patients with resectable head and neck squamous cell carcinoma: a meta-analysis
Abstract
Background: Induction chemotherapy has been investigated as a possible strategy to shrink or downstage locally advanced head and neck cancers, providing opportunity to remove the lesions completely after induction chemotherapy, especially in the patients with resectable advanced disease. The aim of this study was to investigate the definitive effect of induction chemotherapy in patients with resectable head and neck squamous cell carcinoma.
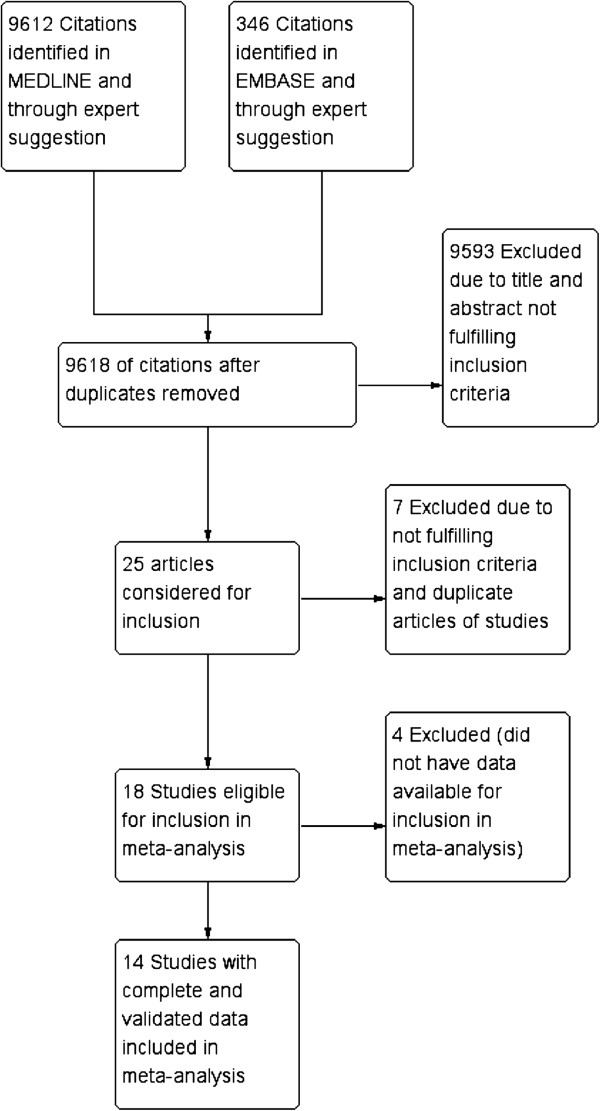
Methods: A meta-analysis of randomized trials (1965-2011) was performed on the impact of induction chemotherapy on survival, disease control, and toxicity in this population of patients. Kaplan-Meier curves were read by Engauge-Digitizer. Data combining was performed using RevMan.
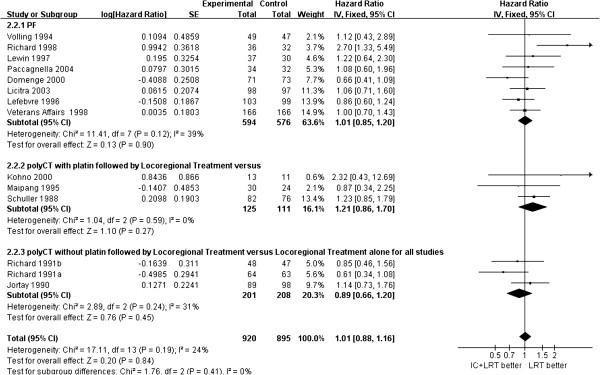
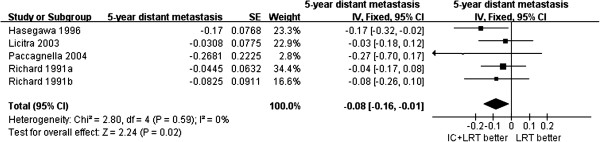
Results: Fourteen trials (2099 patients) were involved in this analysis. There was no significant difference on overall survival, disease free survival, or locoregional recurrence between the patients treated with and without induction chemotherapy (P >0.05). However, the patients treated with induction chemotherapy had a lower rate of distant metastasis by 8% (95% confidence interval 1%-16%, P = 0.02) than those treated without induction chemotherapy. In patients with laryngeal cancer, comparing to radical surgery, the larynx could be preserved in responders to induction chemotherapy without survival decease (P >0.05). Induction chemotherapy-associated death was 0%-5%.
Conclusions: Based on the results above, there is a significant benefit of induction chemotherapy on decreasing distant metastasis in patients with resectable head and neck squamous cell carcinoma. In patients with laryngeal cancer, induction chemotherapy provides larynx preservation in responders to induction chemotherapy.
Figures

References
-
- Forastiere AA. Head and neck cancer: overview of recent developments and future directions. Semin Oncol. 2000;27:1–4. - PubMed
-
- Posner MR, Hershock DM, Blajman CR, Mickiewicz E, Winquist E, Gorbounova V, Tjulandin S, Shin DM, Cullen K, Ervin TJ, Murphy BA, Raez LE, Cohen RB, Spaulding M, Tishler RB, Roth B, Viroglio Rdel C, Venkatesan V, Romanov I, Agarwala S, Harter KW, Dugan M, Cmelak A, Markoe AM, Read PW, Steinbrenner L, Colevas AD, Norris CM Jr, Haddad RI. TAX 324 Study Group. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357:1705–1715. doi: 10.1056/NEJMoa070956. - DOI - PubMed
-
- Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. Lancet. 2000;355:949–955. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
