

DART-bid (Dose-differentiated accelerated radiation therapy, 1.8 Gy twice daily)--a novel approach for non-resected NSCLC: final results of a prospective study, correlating radiation dose to tumor volume
- PMID: 23497555
- PMCID: PMC3606417
- DOI: 10.1186/1748-717X-8-49
DART-bid (Dose-differentiated accelerated radiation therapy, 1.8 Gy twice daily)--a novel approach for non-resected NSCLC: final results of a prospective study, correlating radiation dose to tumor volume
Abstract
Background: Sequential chemo-radiotherapies with intensive radiation components deliver promising results in non-resected non-small cell lung cancer (NSCLC). In general, radiation doses are determined by dose constraints for normal tissues, not by features relevant for tumor control. DART-bid targets directly the doses required for tumor control, correlating doses to tumor volume in a differentiated mode.
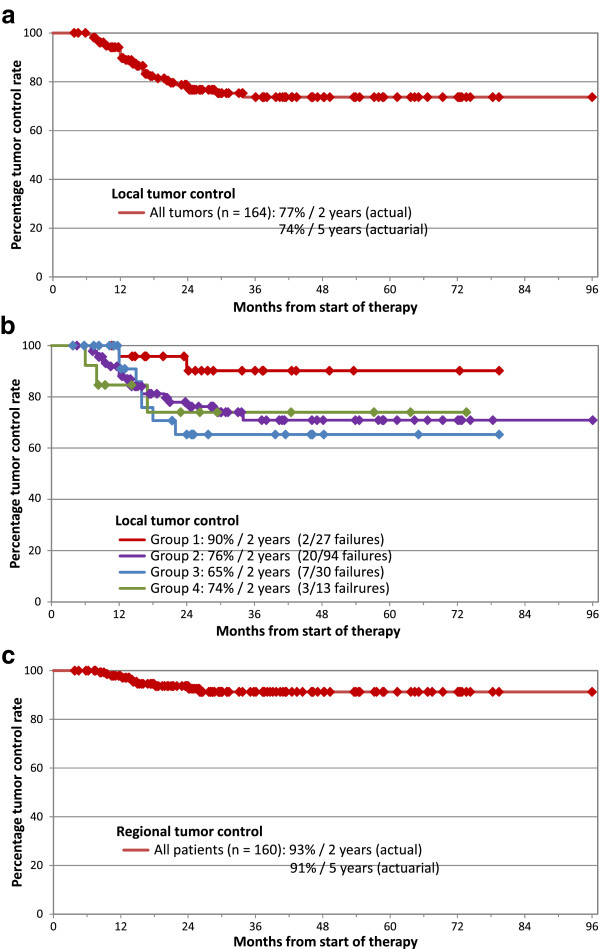
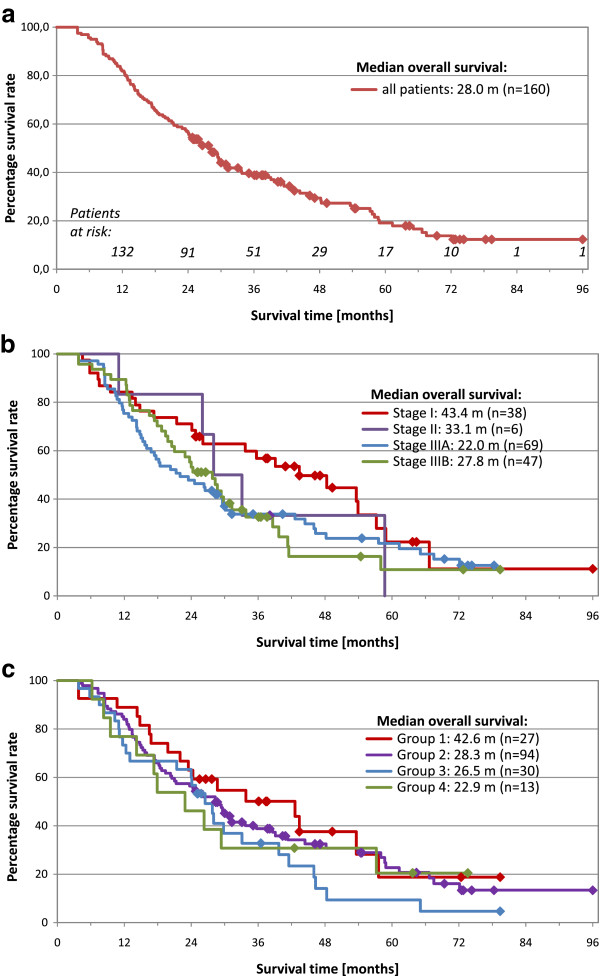
Materials/methods: Radiation doses to primary tumors were aligned along increasing tumor size within 4 groups (<2.5 cm/2.5-4.5 cm/4.5-6.0 cm/>6.0 cm; mean number of three perpendicular diameters). ICRU-doses of 73.8 Gy/79.2 Gy/84.6 Gy/90.0 Gy, respectively, were applied. Macroscopically involved nodes were treated with a median dose of 59.4 Gy, nodal sites about 6 cm cranial to involved nodes electively with 45 Gy. Fractional doses were 1.8 Gy twice daily (bid).2 cycles chemotherapy were given before radiotherapy.Between 2004 and 2009, 160 not selected patients with 164 histologically/cytologically proven NSCLC were enrolled; Stage I: 38 patients; II: 6 pts.; IIIA: 69 pts.; IIIB: 47 pts. Weight loss >5%/3 months: 38 patients (24%).Primary endpoints are local and regional tumor control rates at 2 years (as >90% of locoregional failures occur within 2 years). Secondary endpoints are survival and toxicity. With a minimum follow-up time of 2 years for patients alive, the final results are presented.
Results: 32 local and 10 regional recurrences occurred. The local and regional tumor control rates at 2 years are 77% and 93%, respectively.The median overall survival (OS) time is 28.0 months, the 2- and 5-year OS rates are 57% and 19%, respectively. For stage III patients, median OS amounts to 24.3 months, 2- /5-year OS rates to 51% and 18%, respectively.2 treatment-related deaths (progressive pulmonary fibrosis) occurred in patients with pre-existing pulmonary fibrosis. Further acute and late toxicity was mild.
Conclusions: This novel approach yields a high level of locoregional tumor control and survival times. In general it is well tolerated. In all outcome parameters it seems to compare favourably with simultaneous chemo-radiotherapies, at present considered 'state of the art'; and is additionally amenable for an unselected patient population.
Figures
References
-
- Curran WJ, Paulus R, Langer C, Komaki R, Lee JS, Hauser S, Movsas B, Wasserman T, Rosenthal SA, Gore E, Machtay M, Sause W, Cox JD. Sequential vs. concurrent chemoradiation for stage III non-small lung cancer: Randomized phase III trial RTOG 9410. J Natl Cancer Inst. 2011;103:1452–1460. doi: 10.1093/jnci/djr325. - DOI - PMC - PubMed
-
- Kong FM, Randall K, Ten Haken RK, Schipper MJ, Sullivan MA, Chen M, Lopez C, Kalemkerian GP, Hayman JA. High-dose radiation improved local tumor control and overall survival in patients with inoperable/unresectable non-small cell lung cancer: Long-term results of a radiation dose escalation study. Int J Radiat Oncol Biol Phys. 2005;63:324–333. doi: 10.1016/j.ijrobp.2005.02.010. - DOI - PubMed
-
- Mauguen A, Le Péchoux C, Saunders M, Schild S, Turrisi A, Baumann M, Sause W, Ball D, Belanie C, Bonner J, Zajusz A, Dahlberg S, Nankivell M, Mandrekar S, Paulus R, Behrendt K, Koch R, Bishop J, Dische S, Arriagada R, De Ruysscher D, Pignon JP. Hyperfractionated or accelerated radiotherapy in lung cancer: An individual patient data meta-anlysis. J Clin Oncol. 2012;30:2788–2797. doi: 10.1200/JCO.2012.41.6677. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
