

A comparison of medetomidine and its active enantiomer dexmedetomidine when administered with ketamine in mice
- PMID: 23497612
- PMCID: PMC3605306
- DOI: 10.1186/1746-6148-9-48
A comparison of medetomidine and its active enantiomer dexmedetomidine when administered with ketamine in mice
Abstract
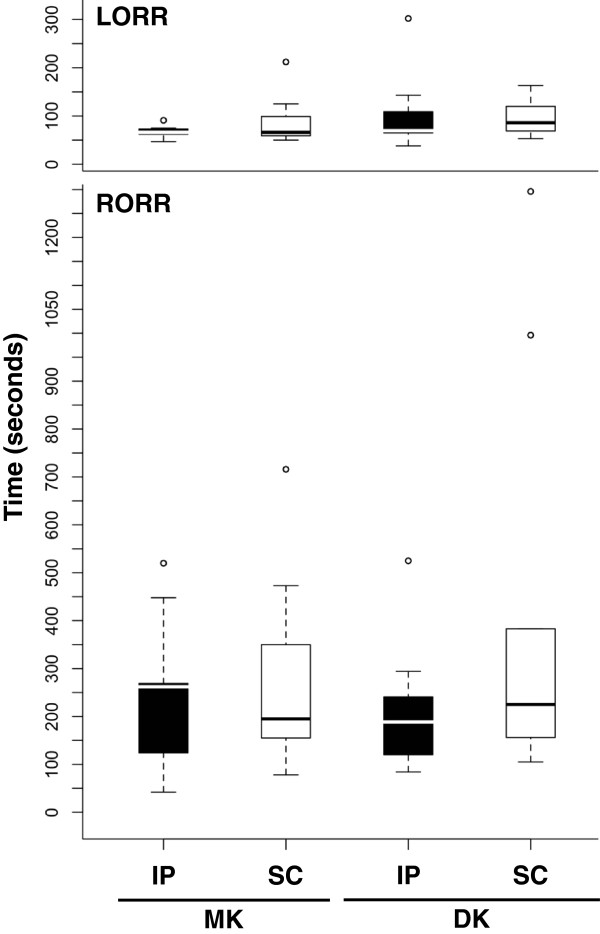
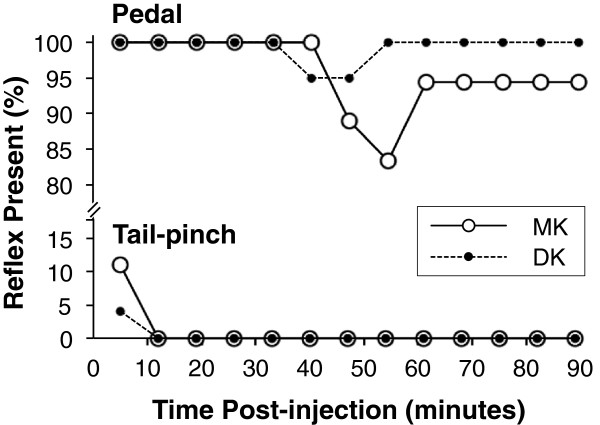
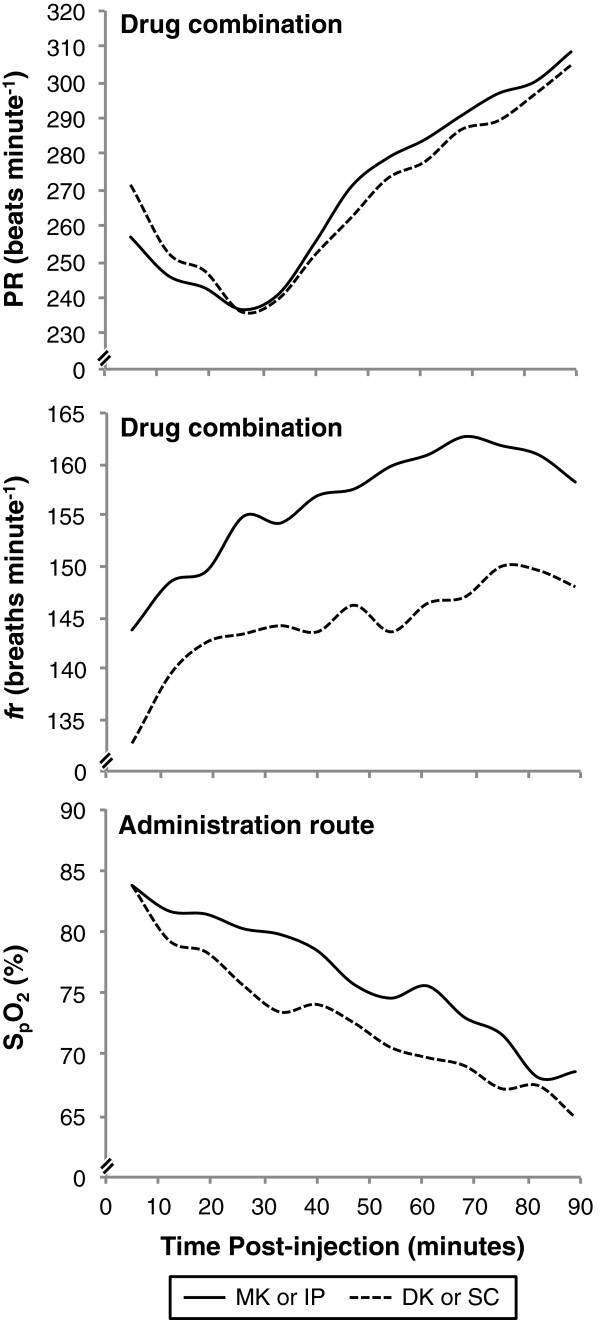
Background: Medetomidine-ketamine (MK) and dexmedetomidine-ketamine (DK) are widely used to provide general anaesthesia in laboratory animals, but have not been compared directly in many of these species, including rodents. This study aimed to compare the onset and depth of anaesthesia, and changes in vital signs, after intraperitoneal (IP) or subcutaneous (SC) administration of ketamine (75 mg kg(-1)) combined with medetomidine (1 mg kg(-1)) or dexmedetomidine (0.5 mg kg(-1)) using a randomised semi-crossover design with ≥ 48 hours between treatments in 10 male and 10 female mice. Each mouse was anaesthetised twice using the same administration route (IP or SC): once with each drug-ketamine combination. Anaesthetised mice were monitored on a heating pad without supplemental oxygen for 89 minutes; atipamezole was administered for reversal. The times that the righting reflex was lost post-injection and returned post-reversal were analysed using general linear models. Tail-pinch and pedal reflexes were examined using binomial generalized linear models. Pulse rate (PR), respiratory rate (fr), and arterial haemoglobin saturation (S(p)O2) were compared using generalized additive mixed models.
Results: There were no significant differences among treatments for the times taken for loss and return of the righting reflex, or response of the tail-pinch reflex. The pedal withdrawal reflex was abolished more frequently with MK than DK over time (P = 0.021). The response of PR and S(p)O2 were similar among treatments, but fr was significantly higher with MK than DK (P ≤ 0.0005). Markedly low S(p)O2 concentrations occurred within 5 minutes post-injection (83.8 ± 6.7%) in all treatment groups and were most severe after 89 minutes lapsed (66.7 ± 7.5%). No statistical differences were detected in regards to administration route (P ≤ 0.94).
Conclusions: This study failed to demonstrate clinical advantages of the enantiomer dexmedetomidine over medetomidine when combined with ketamine to produce general anaesthesia in mice. At the doses administered, deep surgical anaesthesia was not consistently produced with either combination; therefore, anaesthetic depth must be assessed before performing surgical procedures. Supplemental oxygen should always be provided during anaesthesia to prevent hypoxaemia.
Figures
Similar articles
-
General Anesthesia Induced by a Combination of Medetomidine/Vatinoxan with Ketamine and Buprenorphine-ER in C57BL/6J Mice (Mus musculus).J Am Assoc Lab Anim Sci. 2024 Nov 1;63(6):675-682. doi: 10.30802/AALAS-JAALAS-23-000120. J Am Assoc Lab Anim Sci. 2024. PMID: 39237287 Free PMC article.
-
Comparison of S(+)-ketamine and ketamine, with medetomidine, for field anaesthesia in the European brown hare (Lepus europaeus).Vet Anaesth Analg. 2012 Sep;39(5):511-9. doi: 10.1111/j.1467-2995.2012.00754.x. Epub 2012 Jul 13. Vet Anaesth Analg. 2012. PMID: 22788247 Clinical Trial.
-
Assessment of ketamine and medetomidine anaesthesia in the domestic rabbit.Vet Anaesth Analg. 2005 Sep;32(5):271-9. doi: 10.1111/j.1467-2995.2005.00211.x. Vet Anaesth Analg. 2005. PMID: 16135208 Clinical Trial.
-
Classics in Chemical Neuroscience: Medetomidine.ACS Chem Neurosci. 2024 Nov 6;15(21):3874-3883. doi: 10.1021/acschemneuro.4c00583. Epub 2024 Oct 15. ACS Chem Neurosci. 2024. PMID: 39405508 Free PMC article. Review.
-
Consistency in Reporting of Loss of Righting Reflex for Assessment of General Anesthesia in Rats and Mice: A Systematic Review.Comp Med. 2024 Feb 1;74(1):12-18. doi: 10.30802/AALAS-CM-23-000063. Comp Med. 2024. PMID: 38532260 Free PMC article.
Cited by
-
Dose regimens, variability, and complications associated with using repeat-bolus dosing to extend a surgical plane of anesthesia in laboratory mice.J Am Assoc Lab Anim Sci. 2014 Nov;53(6):684-91. J Am Assoc Lab Anim Sci. 2014. PMID: 25650976 Free PMC article.
-
Effects of ketamine, propofol and isoflurane on electrocardiographic variables in clinically healthy dogs premedicated with medetomidine and midazolam.Vet Res Forum. 2024;15(4):187-194. doi: 10.30466/vrf.2024.2008055.3954. Epub 2024 Apr 15. Vet Res Forum. 2024. PMID: 38770200 Free PMC article.
-
A Double-Blinded, Randomized Comparison of Medetomidine-Tiletamine-Zolazepam and Dexmedetomidine-Tiletamine-Zolazepam Anesthesia in Free-Ranging Brown Bears (Ursus Arctos).PLoS One. 2017 Jan 24;12(1):e0170764. doi: 10.1371/journal.pone.0170764. eCollection 2017. PLoS One. 2017. PMID: 28118413 Free PMC article. Clinical Trial.
-
Tamoxifen exacerbates morbidity and mortality in male mice receiving medetomidine anaesthesia.Anim Welf. 2023 Dec 12;32:e78. doi: 10.1017/awf.2023.98. eCollection 2023. Anim Welf. 2023. PMID: 38487465 Free PMC article.
-
Perioperative support reduces mortality of obese BALB/c mice after ovariectomy.Lab Anim (NY). 2016 Jun 21;45(7):262-7. doi: 10.1038/laban.1042. Lab Anim (NY). 2016. PMID: 27327014
References
-
- Arras M, Autenried P, Rettich A, Spaeni D, Rülicke T. Optimization of intraperitoneal injection anesthesia in mice: drugs, dosages, adverse effects and aesthesia depth. Comp Med. 2001;51:443–456. - PubMed
-
- Pypendop B, Serteyn D, Verstegen J. Hemodynamic effects of medetomidine-midazolam-butorphanol combinations and reversibility by atipamezole in dogs. Am J Vet Res. 1996;57:724–730. - PubMed
-
- Savola JM, Virtanen R. Central α2-adrenoceptors are highly stereoselective for dexmedetomidine, the dextro enantiomer of medetomidine. J Pharm. 1991;195:193–199. - PubMed
-
- Meyer RE, Fish RE. In: Anesthesia and Analgesia in Laboratory Animals. 2. Fish RE, Brown MJ, Danneman PJ, Karas AZ, editor. London: Academic Press; 2008. Pharmacology of Injectable Anesthetics, Sedatives, and Tranquilizers; pp. 27–82.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
