

Stereotactic body radiation therapy (SBRT) for clinically localized prostate cancer: the Georgetown University experience
- PMID: 23497695
- PMCID: PMC3610192
- DOI: 10.1186/1748-717X-8-58
Stereotactic body radiation therapy (SBRT) for clinically localized prostate cancer: the Georgetown University experience
Abstract
Background: Stereotactic body radiation therapy (SBRT) delivers fewer high-dose fractions of radiation which may be radiobiologically favorable to conventional low-dose fractions commonly used for prostate cancer radiotherapy. We report our early experience using SBRT for localized prostate cancer.
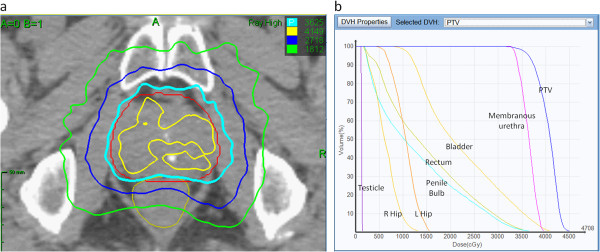
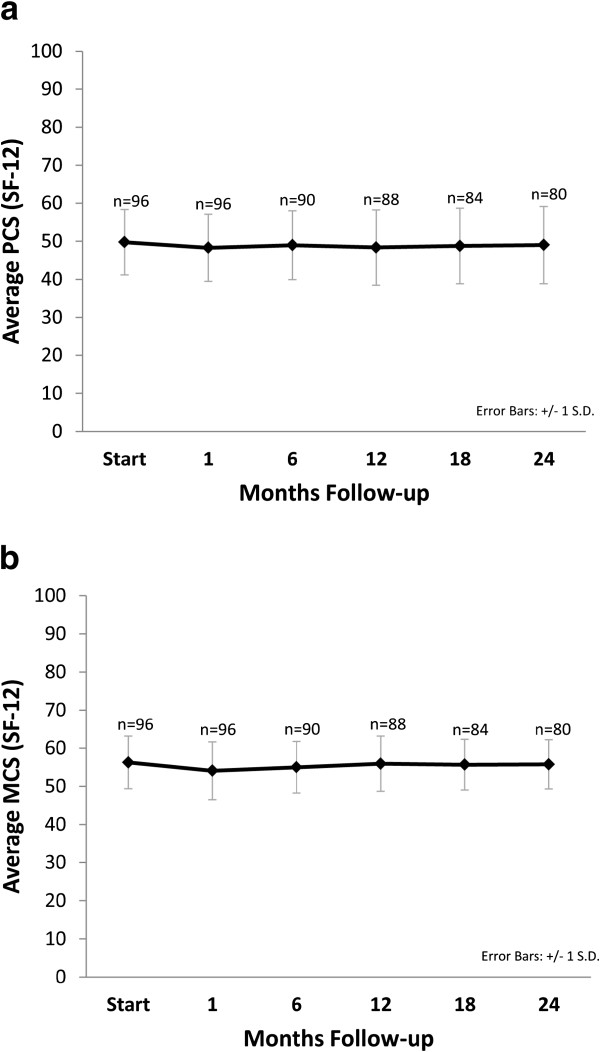
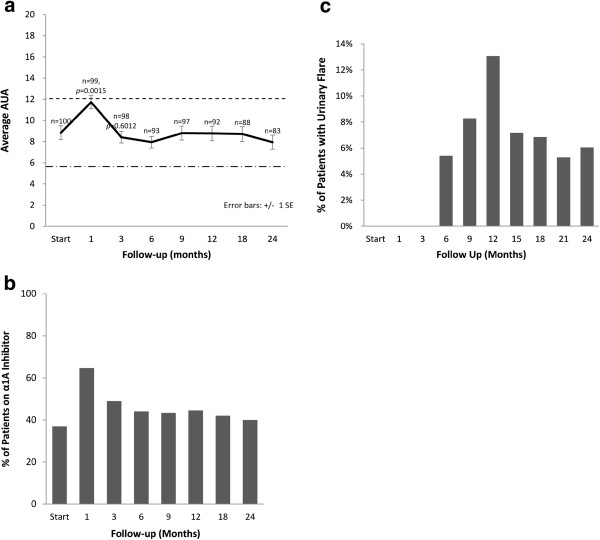
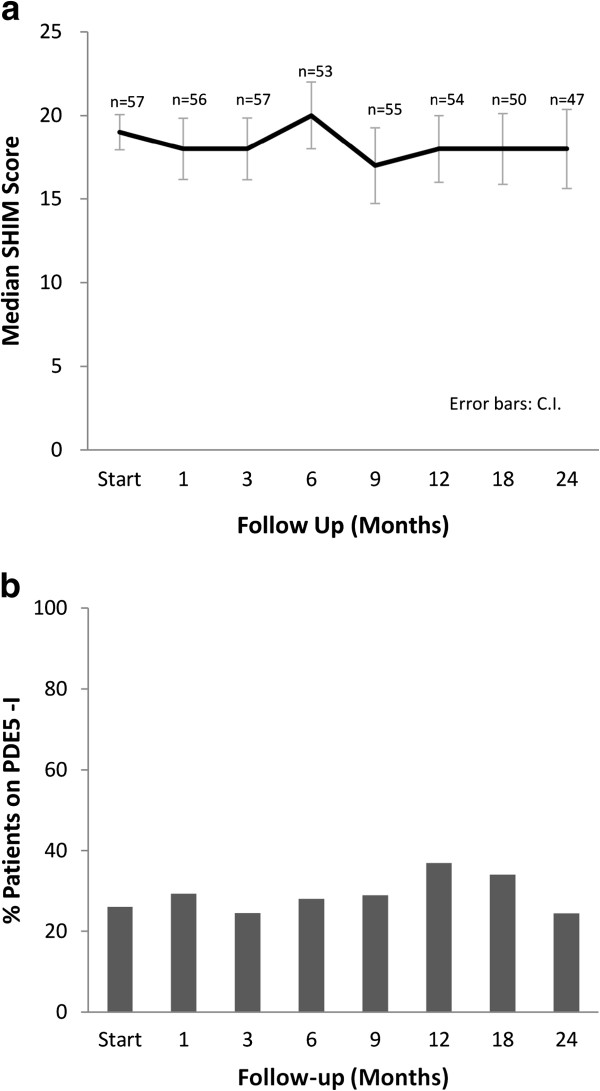
Methods: Patients treated with SBRT from June 2008 to May 2010 at Georgetown University Hospital for localized prostate carcinoma, with or without the use of androgen deprivation therapy (ADT), were included in this retrospective review of data that was prospectively collected in an institutional database. Treatment was delivered using the CyberKnife® with doses of 35 Gy or 36.25 Gy in 5 fractions. Biochemical control was assessed using the Phoenix definition. Toxicities were recorded and scored using the CTCAE v.3. Quality of life was assessed before and after treatment using the Short Form-12 Health Survey (SF-12), the American Urological Association Symptom Score (AUA) and Sexual Health Inventory for Men (SHIM) questionnaires. Late urinary symptom flare was defined as an AUA score ≥ 15 with an increase of ≥ 5 points above baseline six months after the completion of SBRT.
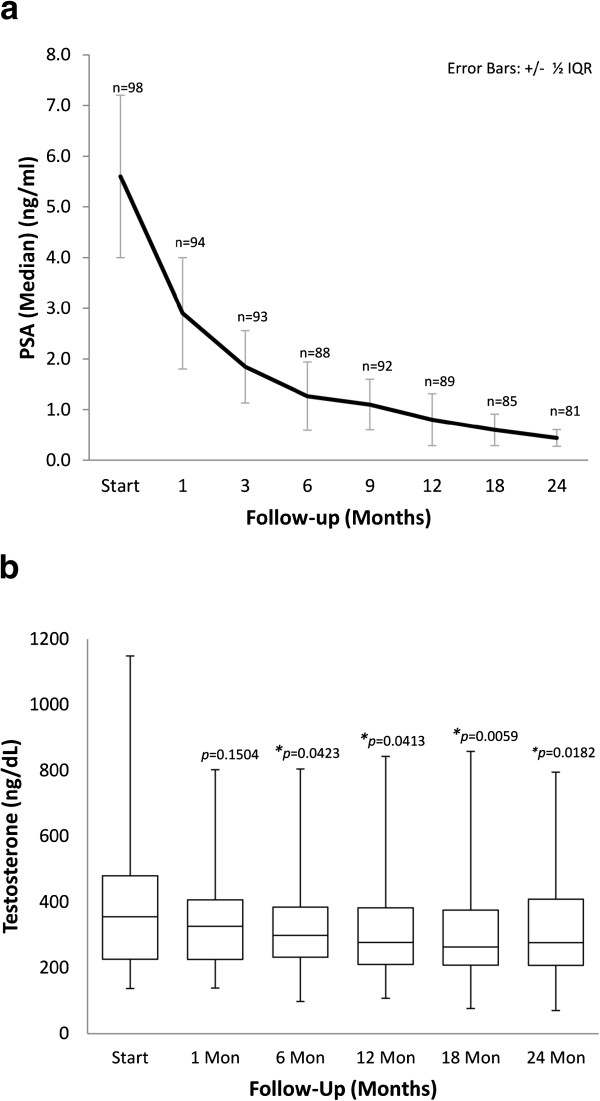
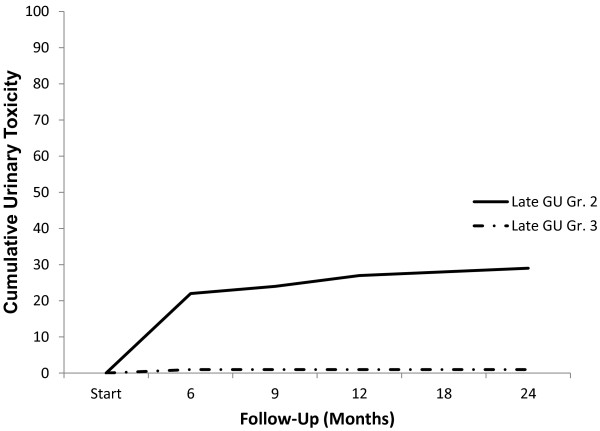
Results: One hundred patients (37 low-, 55 intermediate- and 8 high-risk according to the D'Amico classification) at a median age of 69 years (range, 48-90 years) received SBRT, with 11 patients receiving ADT. The median pre-treatment prostate-specific antigen (PSA) was 6.2 ng/ml (range, 1.9-31.6 ng/ml) and the median follow-up was 2.3 years (range, 1.4-3.5 years). At 2 years, median PSA decreased to 0.49 ng/ml (range, 0.1-1.9 ng/ml). Benign PSA bounce occurred in 31% of patients. There was one biochemical failure in a high-risk patient, yielding a two-year actuarial biochemical relapse free survival of 99%. The 2-year actuarial incidence rates of GI and GU toxicity ≥ grade 2 were 1% and 31%, respectively. A median baseline AUA symptom score of 8 significantly increased to 11 at 1 month (p=0.001), however returned to baseline at 3 months (p=0.60). Twenty one percent of patients experienced a late transient urinary symptom flare in the first two years following treatment. Of patients who were sexually potent prior to treatment, 79% maintained potency at 2 years post-treatment.
Conclusions: SBRT for clinically localized prostate cancer was well tolerated, with an early biochemical response similar to other radiation therapy treatments. Benign PSA bounces were common. Late GI and GU toxicity rates were comparable to conventionally fractionated radiation therapy and brachytherapy. Late urinary symptom flares were observed but the majority resolved with conservative management. A high percentage of men who were potent prior to treatment remained potent two years following treatment.
Figures
References
-
- Madsen BL, Hsi RA, Pham HT, Fowler JF, Esagui L, Corman J. Stereotactic hypofractionated accurate radiotherapy of the prostate (SHARP), 33.5 Gy in five fractions for localized disease: first clinical trial results. Int J Radiat Oncol Biol Phys. 2007;67:1099–1105. doi: 10.1016/j.ijrobp.2006.10.050. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
