

Inducible myocardial ischemia and outcomes in patients with coronary artery disease and left ventricular dysfunction
- PMID: 23500234
- PMCID: PMC3755503
- DOI: 10.1016/j.jacc.2013.02.014
Inducible myocardial ischemia and outcomes in patients with coronary artery disease and left ventricular dysfunction
Abstract
Objectives: The study objectives were to test the hypotheses that ischemia during stress testing has prognostic value and identifies those patients with coronary artery disease (CAD) with left ventricular (LV) dysfunction who derive the greatest benefit from coronary artery bypass grafting (CABG) compared with medical therapy.
Background: The clinical significance of stress-induced ischemia in patients with CAD and moderately to severely reduced LV ejection fraction (EF) is largely unknown.
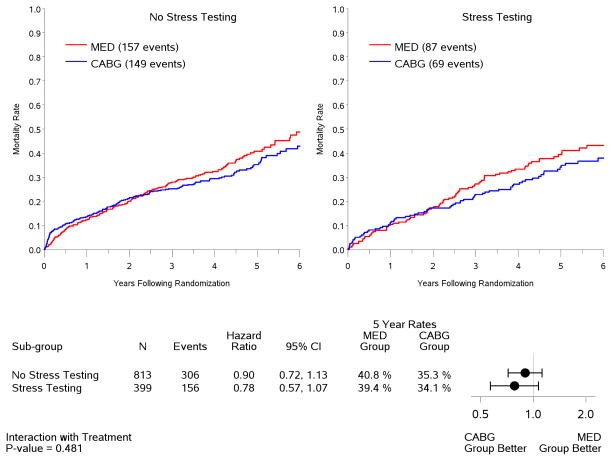
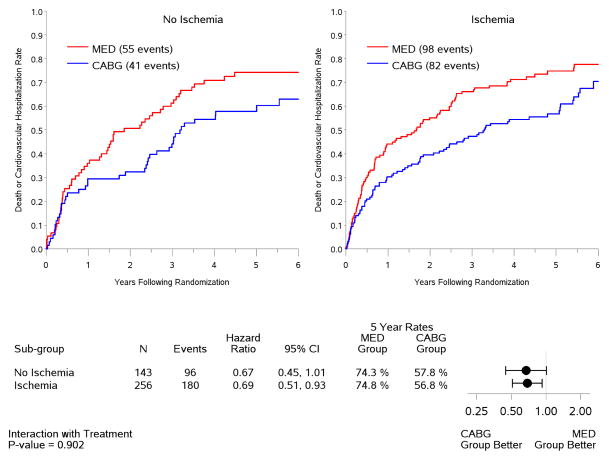
Methods: The STICH (Surgical Treatment for IsChemic Heart Failure) trial randomized patients with CAD and EF ≤35% to CABG or medical therapy. In the current study, we assessed the outcomes of those STICH patients who underwent a radionuclide (RN) stress test or a dobutamine stress echocardiogram (DSE). A test was considered positive for ischemia by RN testing if the summed difference score (difference in tracer activity between stress and rest) was ≥4 or if ≥2 of 16 segments were ischemic during DSE. Clinical endpoints were assessed by intention to treat during a median follow-up of 56 months.
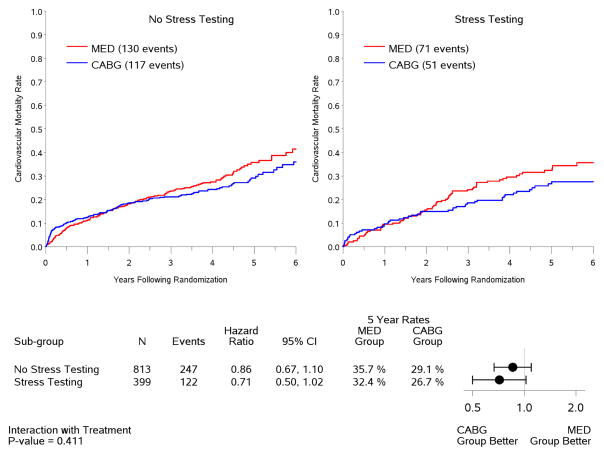
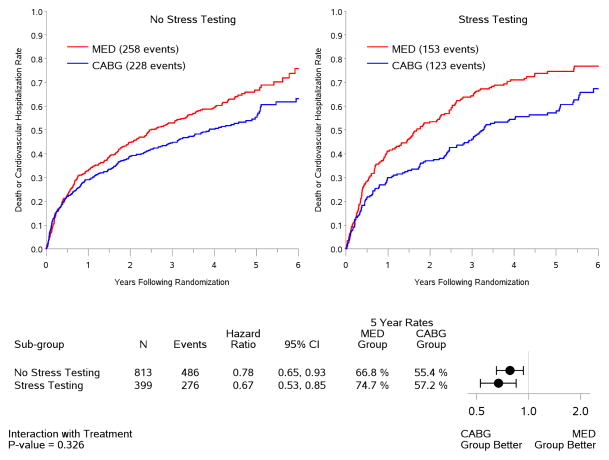
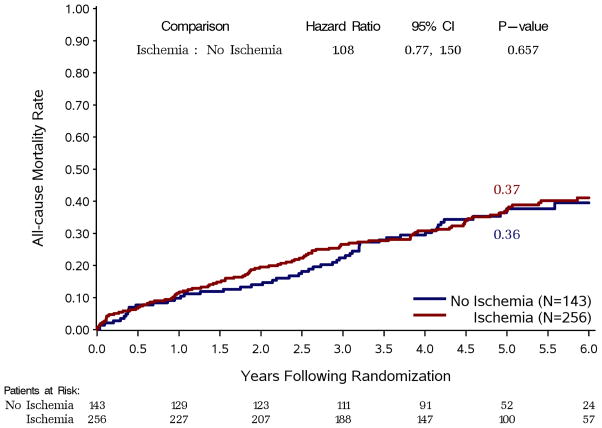
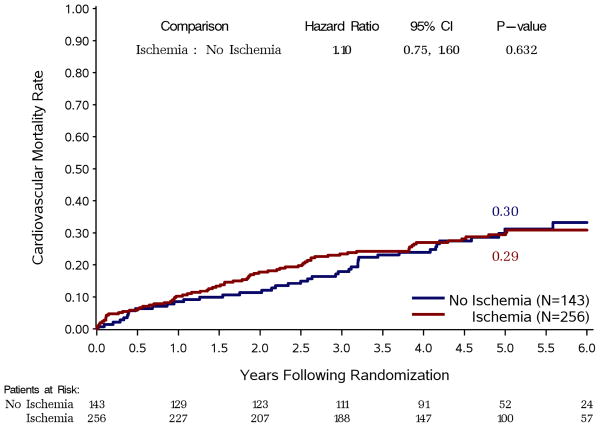
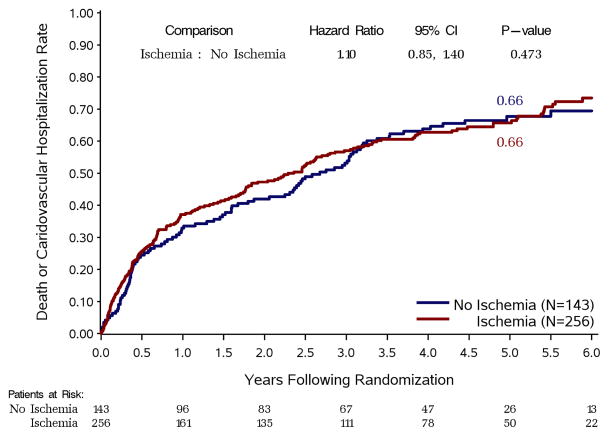
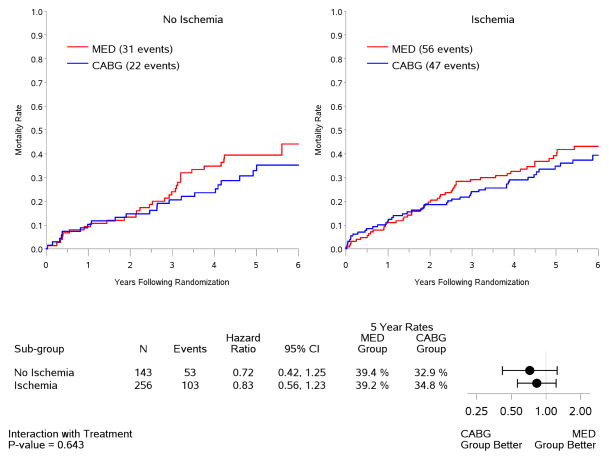
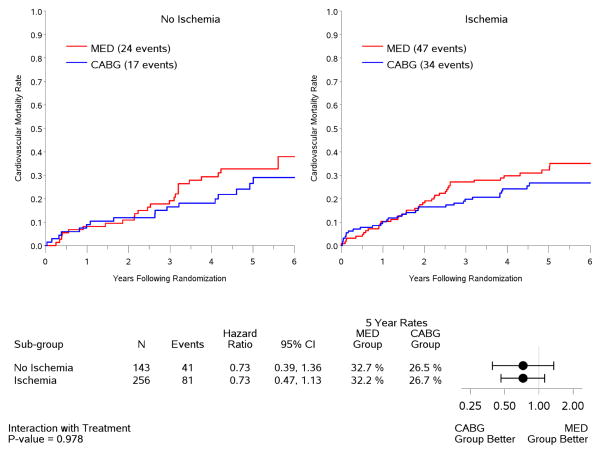
Results: Of the 399 study patients (51 women, mean EF 26 ± 8%), 197 were randomized to CABG and 202 were randomized to medical therapy. Myocardial ischemia was induced during stress testing in 256 patients (64% of the study population). Patients with and without ischemia were similar in age, multivessel CAD, previous myocardial infarction, LV EF, LV volumes, and treatment allocation (all p = NS). There was no difference between patients with and without ischemia in all-cause mortality (hazard ratio: 1.08; 95% confidence interval: 0.77 to 1.50; p = 0.66), cardiovascular mortality, or all-cause mortality plus cardiovascular hospitalization. There was no interaction between ischemia and treatment for any clinical endpoint.
Conclusions: In CAD with severe LV dysfunction, inducible myocardial ischemia does not identify patients with worse prognosis or those with greater benefit from CABG over optimal medical therapy. (Comparison of Surgical and Medical Treatment for Congestive Heart Failure and Coronary Artery Disease [STICH]; NCT00023595).
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Is ischemia dead after STICH?J Am Coll Cardiol. 2013 May 7;61(18):1871-3. doi: 10.1016/j.jacc.2013.02.018. Epub 2013 Mar 7. J Am Coll Cardiol. 2013. PMID: 23500324 No abstract available.
-
Reply: Is ischemia really bad for you?J Am Coll Cardiol. 2013 Dec 3;62(22):2149. doi: 10.1016/j.jacc.2013.07.060. Epub 2013 Aug 28. J Am Coll Cardiol. 2013. PMID: 23994400 No abstract available.
-
Is ischemia really bad for you?J Am Coll Cardiol. 2013 Dec 3;62(22):2148-9. doi: 10.1016/j.jacc.2013.06.056. Epub 2013 Aug 28. J Am Coll Cardiol. 2013. PMID: 23994408 No abstract available.
References
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease. J Am Coll Cardiol. 2012;60:2564–603. - PubMed
-
- Fox K, Garcia MAA, Ardissino D, et al. Guidelines on the management of stable angina pectoris: executive summary. The task force on the management of stable angina pectoris of the European Society of Cardiology. Eur Heart J. 2006;27:1341–81. - PubMed
-
- Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2012;59:857–81. - PubMed
-
- Weiner DA, Ryan TJ, McCabe CH, et al. The role of exercise testing in identifying patients with improved survival after coronary artery bypass surgery. J Am Coll Cardio. 1986;8:741–8. - PubMed
-
- Shaw LJ, Berman DS, Maron DJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–91. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
