

Outcomes associated with microalbuminuria: effect modification by chronic kidney disease
- PMID: 23500283
- PMCID: PMC3625505
- DOI: 10.1016/j.jacc.2012.11.071
Outcomes associated with microalbuminuria: effect modification by chronic kidney disease
Abstract
Objectives: This study sought to compare the association of microalbuminuria with outcomes in patients with different comorbidities.
Background: The risk of adverse outcomes associated with lower levels proteinuria has been found to be linearly decreasing with even low-normal levels of microalbuminuria. It is unclear whether comorbid conditions change these associations.
Methods: We examined the association of urine microalbumin-creatinine ratio (UACR) with mortality and the slopes of estimated glomerular filtration rate (eGFR) in a nationally representative cohort of 298,875 U.S. veterans. Associations of UACR with all-cause mortality overall and in subgroups of patients with and without diabetes mellitus, hypertension, cardiovascular disease, congestive heart failure, and advanced chronic kidney disease (CKD) were examined in Cox models, and with the slopes of eGFR in linear and logistic regression models.
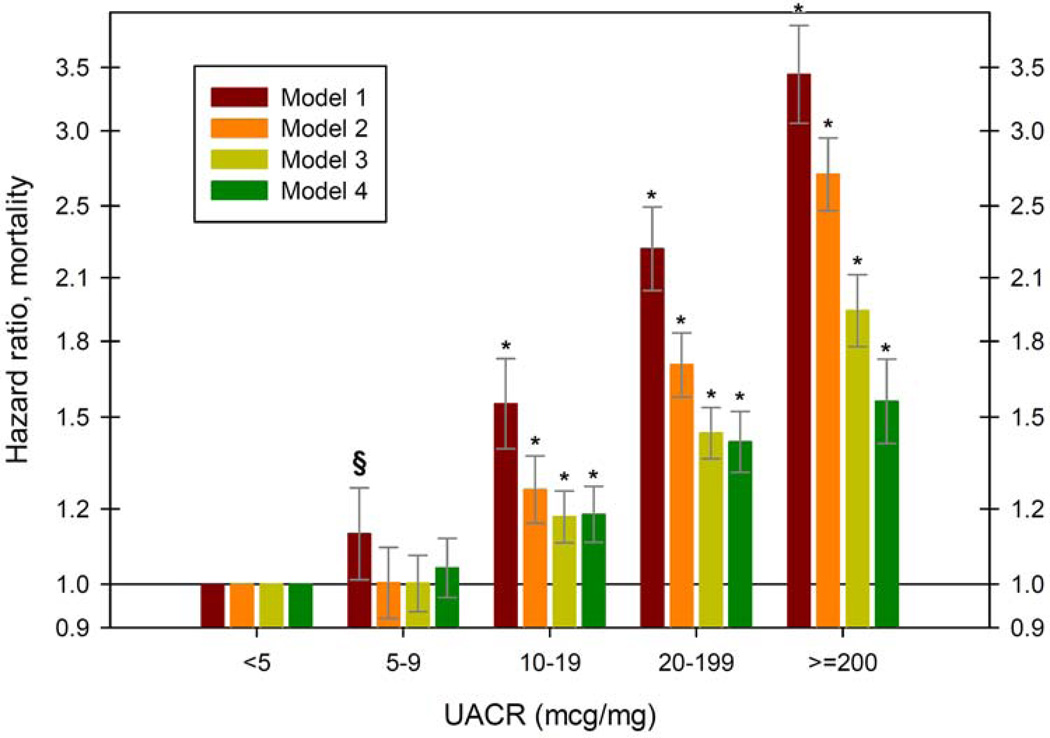
Results: Very low levels of UACR were linearly associated with decreased mortality and less progression of CKD overall: adjusted mortality hazard ratio and estimated glomerular filtration rate slope (95% confidence interval [CI]) associated with UACR ≥200 μg/mg, compared to <5 μg/mg were 1.53 (95% CI: 1.38 to 1.69, p < 0.001) and -1.59 (95% CI: -1.83 to -1.35, p < 0.001). Similar linearity was present in all examined subgroups, except in patients with CKD in whom a U-shaped association was present and in whom a UACR of 10 to 19 was associated with the best outcomes.
Conclusions: The association of UACR with mortality and with progressive CKD is modified in patients with CKD, who experience higher mortality and worse progression of CKD with the lowest levels of UACR. Proteinuria-lowering interventions in patients with advanced CKD should be implemented cautiously, considering the potential for adverse outcomes.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Albuminuria in the normal range: the lower is not the better.J Am Coll Cardiol. 2013 Apr 16;61(15):1634-6. doi: 10.1016/j.jacc.2013.01.049. J Am Coll Cardiol. 2013. PMID: 23500278 No abstract available.
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Hillege HL, Fidler V, Diercks GF, et al. Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation. 2002;106:1777–1882. - PubMed
-
- Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, et al. Very low levels of microalbuminuria are associated with increased risk of coronary heart disease and death independently of renal function, hypertension, and diabetes. Circulation. 2004;110:32–35. - PubMed
-
- Romundstad S, Holmen J, Kvenild K, Hallan H, Ellekjaer H. Microalbuminuria and all-cause mortality in 2,089 apparently healthy individuals: a 4.4-year follow-up study. The Nord-Trondelag Health Study (HUNT), Norway. Am J Kidney Dis. 2003;42:466–473. - PubMed
-
- Yuyun MF, Khaw KT, Luben R, et al. Microalbuminuria independently predicts all-cause and cardiovascular mortality in a British population: The European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) population study. Int J Epidemiol. 2004;33:189–198. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
