

Heart failure–associated hospitalizations in the United States
- PMID: 23500328
- PMCID: PMC3838728
- DOI: 10.1016/j.jacc.2012.12.038
Heart failure–associated hospitalizations in the United States
Abstract
Objectives: This study sought to characterize temporal trends in hospitalizations with heart failure as a primary or secondary diagnosis.
Background: Heart failure patients are frequently admitted for both heart failure and other causes.
Methods: Using the Nationwide Inpatient Sample (NIS), we evaluated trends in heart failure hospitalizations between 2001 and 2009. Hospitalizations were categorized as either primary or secondary heart failure hospitalizations based on the location of heart failure in the discharge diagnosis. National estimates were calculated using the sampling weights of the NIS. Age- and sex-standardized hospitalization rates were determined by dividing the number of hospitalizations by the U.S. population in a given year and using direct standardization.
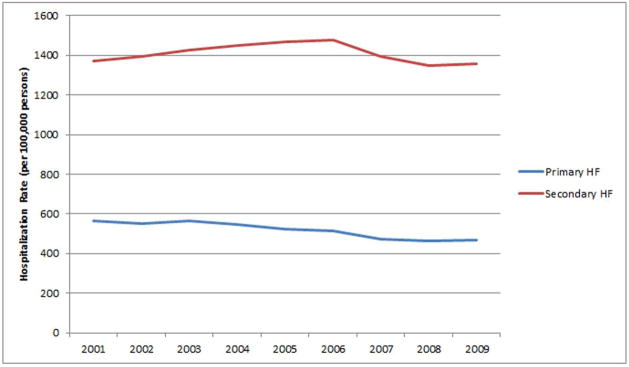
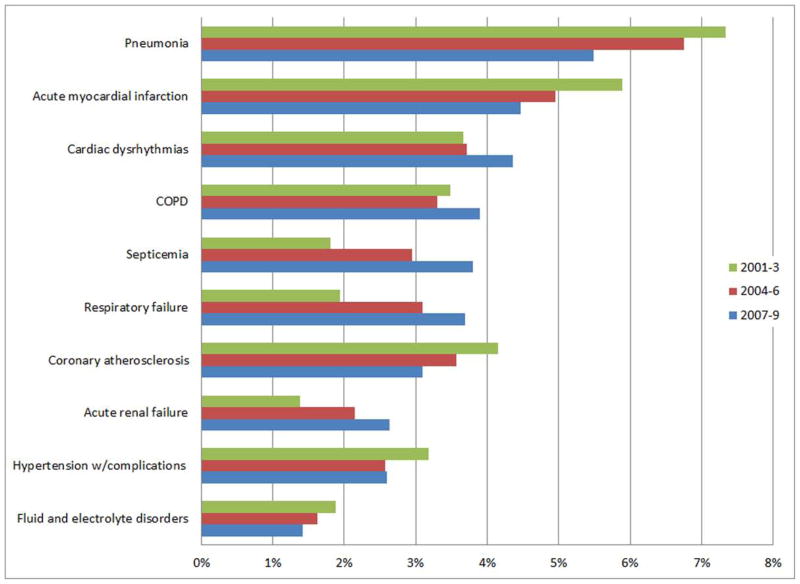
Results: The number of primary heart failure hospitalizations in the United States decreased from 1,137,944 in 2001 to 1,086,685 in 2009, whereas secondary heart failure hospitalizations increased from 2,753,793 to 3,158,179 over the same period. Age- and sex-adjusted rates of primary heart failure hospitalizations decreased steadily from 2001 to 2009, from 566 to 468 per 100,000 people. Rates of secondary heart failure hospitalizations initially increased from 1,370 to 1,476 per 100,000 people from 2001 to 2006, then decreased to 1,359 per 100,000 people in 2009. Common primary diagnoses for secondary heart failure hospitalizations included pulmonary disease, renal failure, and infections.
Conclusions: Although primary heart failure hospitalizations declined, rates of hospitalizations with a secondary diagnosis of heart failure were stable in the past decade. Strategies to reduce the high burden of hospitalizations of heart failure patients should include consideration of both cardiac disease and noncardiac conditions.
Figures
Comment in
-
The changing landscape of heart failure hospitalizations.J Am Coll Cardiol. 2013 Mar 26;61(12):1268-70. doi: 10.1016/j.jacc.2013.01.011. J Am Coll Cardiol. 2013. PMID: 23500329 No abstract available.
References
-
- Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA. 1995;273:1450–6. - PubMed
-
- Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348:1309–21. - PubMed
-
- Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341:709–17. - PubMed
-
- Hjalmarson A, Goldstein S, Fagerberg B, et al. Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure: the Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). MERIT-HF Study Group. JAMA. 2000;283:1295–302. - PubMed
-
- Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. U.S. Carvedilol Heart Failure Study Group. N Engl J Med. 1996;334:1349–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
