

Rare small bowel obstruction: Right paraduodenal hernia. Case report
- PMID: 23500746
- PMCID: PMC3604702
- DOI: 10.1016/j.ijscr.2012.11.027
Rare small bowel obstruction: Right paraduodenal hernia. Case report
Abstract
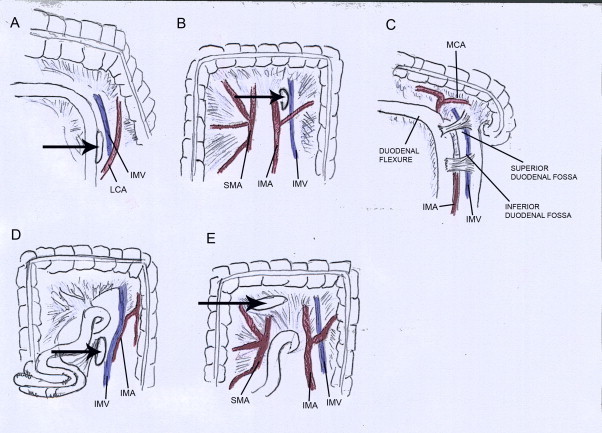
Introduction: Paraduodenal hernia (paramesocolic hernia), a rare congenital anomaly due to a midgut malrotation during fetal development, is recognized as the most frequent internal hernias. Two variants have been described: left and right, the latter less common than the first one.
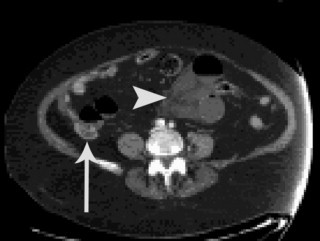
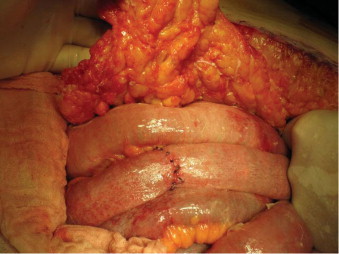
Presentation of case: We report a right paraduodenal hernia case in a 86 years old female patient who developed an acute bowel obstruction syndrome. Final diagnosis was achieved by imaging techniques as abdomen X-ray and CT and confirmed only after surgical operation.
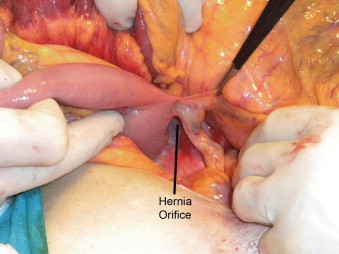
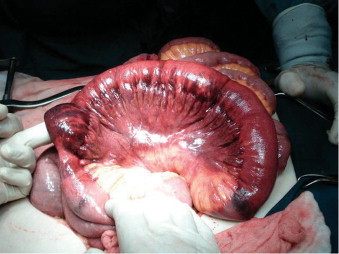
Discussion: Surgical approach was via median laparotomy, consisting in hernia reduction, replacement and stitching of the bowel in its anatomical orientation, and fixing of the posterior wall defect. At 15 months follow-up from surgical procedure the patient is asymptomatic.
Conclusion: Paraduodenal hernia is a rare pathology but its involvement in bowel obstruction syndrome should be always taken into account during diagnostic process.
Copyright © 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Stern L.E., Warner B.W. Congenital internal abdominal hernias: incidence and management. In: Fitzgibbons R.J., Greenburg A.G., editors. Nyhus and condon's hernia. 5th ed. Lippincott Williams and Wilkins; Philadelphia: 2002.
-
- Treitz W. Credner; Prague: 1857. Hernia retroperitonealis. Ein Beitrag zur Geschichte innerer Hernien.
-
- Jonnesco T. Legrosnier et Babe; Paris: 1889. Anatomie topographique du duodenum et hernies duodenales.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
