

The clustering of cardiovascular disease risk factors and their impacts on annual medical expenditure in Japan: community-based cost analysis using Gamma regression models
- PMID: 23503577
- PMCID: PMC3612762
- DOI: 10.1136/bmjopen-2012-002234
The clustering of cardiovascular disease risk factors and their impacts on annual medical expenditure in Japan: community-based cost analysis using Gamma regression models
Abstract
Objective: The clustering of cardiovascular disease (CVD) risk factors is a serious threat for increasing medical expenses. The age-specific proportion and distribution of medical expenditure attributable to CVD risk factors, especially focused on the elderly, is thus indispensable for formulating public health policy given the extent of the ageing population in developed countries.
Design: Cost analysis using individuals' medical expenses and their corresponding health examination measures.
Setting: Shiga prefecture, Japan, from April 2000 to March 2006.
Participants: 33 213 participants aged 40 years and over.
Main outcome measures: Mean medical expenditure per year.
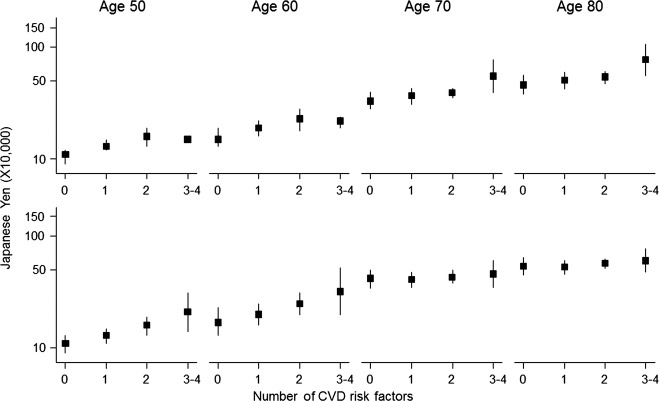
Methods: Gamma regression models were applied to examine how the number of CVD risk factors affects mean medical expenditure. The four CVD risk factors analysed in this study were defined as follows: hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg), hypercholesterolaemia (serum total cholesterol ≥240 mg/dl), high blood glucose (casual blood glucose ≥200 mg/dl) and smoking (current smoker). Sex-specific and age-specific investigations were carried out on the elderly (aged 65 and over) and non-elderly (aged 40-64) populations.
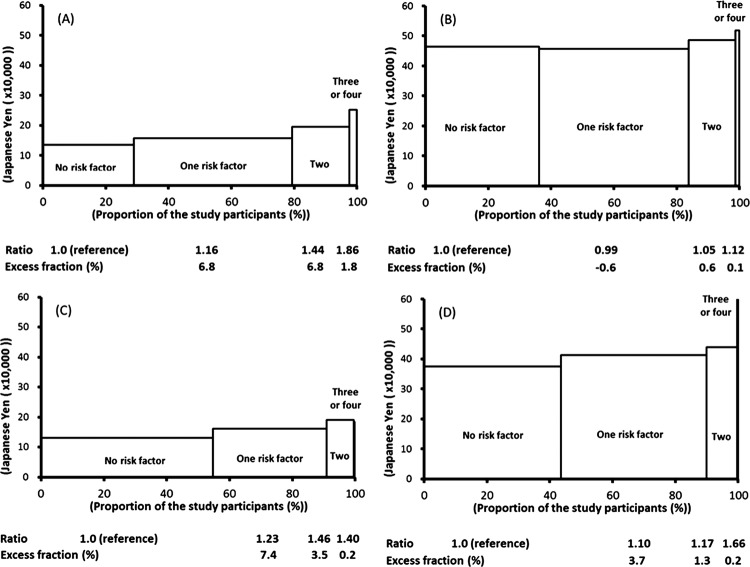
Results: The mean medical expenditure (per year) for the no CVD risk-factor group was only 110 000 yen at age 50 (men, 110 708 yen; women, 107 109 yen), but this expenditure was 6-7 times higher for 80-year-olds who have three or four CVD risk factors (men, 603 351 yen; women, 765 673 yen). The total overspend (excess fraction) was larger for the non-elderly (men, 15.4%; women, 11.1%) than that for the elderly (men, 0.1%; women, 5.2%) and largely driven by people with one or two CVD risk factors, except for elderly men.
Conclusions: The age-specific proportion and distribution of medical expenditure attributable to CVD risk factors showed that a high-risk approach for the elderly and a population approach for the majority are both necessary to reduce total medical expenditure in Japan.
Figures
References
-
- Ezzati M, Hoorn SV, Rodgers A, et al. Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet 2003;362:271–80 - PubMed
-
- Greenland P, Knoll MD, Stamler J, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA 2003;290:891–7 - PubMed
-
- Kadota A, Hozawa A, Okamura T, et al. Relationship between metabolic risk factor clustering and cardiovascular mortality stratified by high blood glucose and obesity: NIPPON DATA90, 1990–2000. Diabetes Care 2007;30:1533–8 - PubMed
-
- McNeill AM, Rosamond WD, Girman CJ, et al. The metabolic syndrome and 11-year risk of incident cardiovascular disease in the atherosclerosis risk in communities study. Diabetes Care 2005;28:385–90 - PubMed
-
- Nakamura K, Okamura T, Kanda H, et al. Medical costs of patients with hypertension and/or diabetes: a 10-year follow-up study of national health insurance in Shiga, Japan. J Hypertens 2006;24:2305–9 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous