

Renal dysfunction in STEMI-patients undergoing primary angioplasty: higher prevalence but equal prognostic impact in female patients; an observational cohort study from the Belgian STEMI registry
- PMID: 23506004
- PMCID: PMC3635996
- DOI: 10.1186/1471-2369-14-62
Renal dysfunction in STEMI-patients undergoing primary angioplasty: higher prevalence but equal prognostic impact in female patients; an observational cohort study from the Belgian STEMI registry
Abstract
Background: Mortality in female patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary angioplasty (pPCI) is higher than in men. We examined gender differences in the prevalence and prognostic performance of renal dysfunction at admission in this setting.
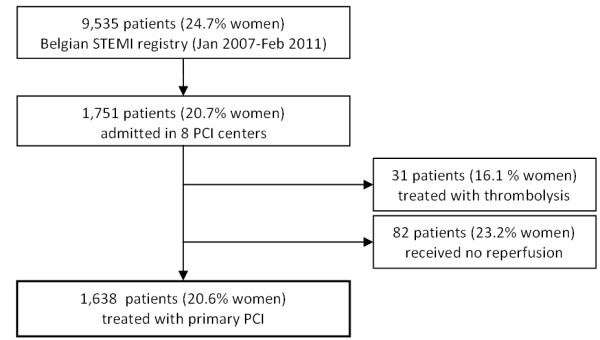
Methods: A multicenter retrospective sub-analysis of the Belgian STEMI-registry identified 1,638 patients (20.6% women, 79.4% men) treated with pPCI in 8 tertiary care hospitals (January 2007-February 2011). The estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI equation. Main outcome measure was in-hospital mortality.
Results: More women than men suffered from renal dysfunction at admission (42.3% vs. 25.3%, p < 0.001). Mortality in women was doubled as compared to men (9.5 vs. 4.7%, OR (95% CI) = 2.12 (1.36-3.32), p<0.001). In-hospital mortality for men and women with vs. without renal dysfunction was much higher (10.7 and 15.3 vs. 2.3 and 2.4%, p < 0.001). In a multivariable regression analysis, adjusting for age, gender, peripheral artery disease (PAD), coronary artery disease (CAD), hypertension, diabetes and low body weight (<67 kg), female gender was associated with renal dysfunction at admission (OR (95% CI) 1.65 (1.20-2.25), p = 0.002). In a multivariable model including TIMI risk score and renal dysfunction, renal dysfunction was an independent predictor of in-hospital mortality in both men (OR (95% CI) = 2.39 (1.27-4.51), p = 0.007) and women (OR (95% CI) = 4.03 (1.26-12.92), p = 0.02), with a comparable impact for men and women (p for interaction = 0.69).
Conclusions: Female gender was independently associated with renal dysfunction at admission in pPCI treated patients. Renal dysfunction was equally associated with higher in-hospital mortality in both men and women.
Figures


References
-
- De Luca G, Gibson CM, Gyongyosi M, Zeymer U, Dudek D, Arntz HR, Bellandi F, Maioli M, Noc M, Zorman S, Gabriel HM, Emre A, Cutlip D, Rakowski T, Huber K, van’t Hof AW. Gender-related differences in outcome after ST-segment elevation myocardial infarction treated by primary angioplasty and glycoprotein IIb-IIIa inhibitors: insights from the EGYPT cooperation. J Thromb Thrombolysis. 2010;30:342–346. doi: 10.1007/s11239-010-0451-y. - DOI - PubMed
-
- Zhang Q, Qiu JP, Zhang RY, Li YG, He B, Jin HG, Zhang JF, Wang XL, Jiang L, Liao ML, Hu J, Shen WF. Absence of gender disparity in short-term clinical outcomes in patients with acute ST-segment elevation myocardial infarction undergoing sirolimus-eluting stent based primary coronary intervention: a report from Shanghai Acute Coronary Event (SACE) Registry. Chin Med J (Engl) 2010;123:782–788. - PubMed
-
- Sjauw KD, Stegenga NK, Engstrom AE, van der Schaaf RJ, Vis MM, Macleod A, Baan JJ, Koch KT, de Winter RJ, Tijssen JG, Piek JJ, Henriques JP. The influence of gender on short- and long-term outcome after primary PCI and delivered medical care for ST-segment elevation myocardial infarction. EuroIntervention. 2010;5:780–787. doi: 10.4244/EIJV5I7A131. - DOI - PubMed
-
- Jackson EA, Moscucci M, Smith DE, Share D, Dixon S, Greenbaum A, Grossman PM, Gurm HS. The association of sex with outcomes among patients undergoing primary percutaneous coronary intervention for ST elevation myocardial infarction in the contemporary era: Insights from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2) Am Heart J. 2011;161:106–112. doi: 10.1016/j.ahj.2010.09.030. e1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
