

Temporal trends of molecular markers associated with artemether-lumefantrine tolerance/resistance in Bagamoyo district, Tanzania
- PMID: 23506218
- PMCID: PMC3732084
- DOI: 10.1186/1475-2875-12-103
Temporal trends of molecular markers associated with artemether-lumefantrine tolerance/resistance in Bagamoyo district, Tanzania
Abstract
Background: Development and spread of Plasmodium falciparum resistance to artemisinin-based combination therapy (ACT) constitutes a major threat to recent global malaria control achievements. Surveillance of molecular markers could act as an early warning system of ACT-resistance before clinical treatment failures are apparent. The aim of this study was to analyse temporal trends of established genotypes associated with artemether-lumefantrine tolerance/resistance before and after its deployment as first-line treatment for uncomplicated malaria in Tanzania 2006.
Methods: Single nucleotide polymorphisms in the P. falciparum multidrug resistance gene 1 (pfmdr1) N86Y, Y184F, D1246Y and P. falciparum chloroquine transporter gene (pfcrt) K76T were analysed from dried blood spots collected during six consecutive studies from children with uncomplicated P. falciparum malaria in Fukayosi village, Bagamoyo District, Tanzania, between 2004-2011.
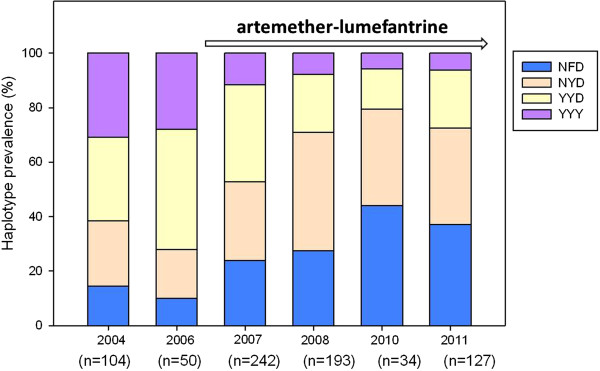
Results: There was a statistically significant yearly increase of pfmdr1 N86, 184F, D1246 and pfcrt K76 between 2006-2011 from 14% to 61% (yearly OR = 1.38 [95% CI 1.25-1.52] p < 0.0001), 14% to 35% (OR = 1.17 [95% CI 1.07-1.30] p = 0.001), 54% to 85% (OR = 1.21 [95% CI 1.03-1.42] p = 0.016) and 49% to 85% (OR = 1.33 [95% CI 1.17-1.51] p < 0.0001), respectively. Unlike for the pfmdr1 SNP, a significant increase of pfcrt K76 was observed already between 2004-2006, from 26% to 49% (OR = 1.68 [95% CI 1.17-2.40] p = 0.005). From 2006 to 2011 the pfmdr1 NFD haplotype increased from 10% to 37% (OR = 1.25 [95% CI 1.12-1.39] p < 0.0001), whereas the YYY haplotype decreased from 31% to 6% (OR = 0.73 [95% CI 0.56-0.98] p = 0.018). All 390 successfully analysed samples had one copy of the pfmdr1 gene.
Conclusion: The temporal selection of molecular markers associated with artemether-lumefantrine tolerance/resistance may represent an early warning sign of impaired future drug efficacy. This calls for stringent surveillance of artemether-lumefantrine efficacy in Tanzania and emphasizes the importance of molecular surveillance as a complement to standard in vivo trials.
Figures

References
-
- Amaratunga C, Sreng S, Suon S, Phelps ES, Stepniewska K, Lim P, Zhou C, Mao S, Anderson JM, Lindegardh N, Jiang H, Song J, Su XZ, White NJ, Dondorp AM, Anderson TJ, Fay MP, Mu J, Duong S, Fairhurst RM. Artemisinin-resistant Plasmodium falciparum in Pursat province, western Cambodia: a parasite clearance rate study. Lancet Infect Dis. 2012;12:851–858. - PMC - PubMed
-
- Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, Lwin KM, Ariey F, Hanpithakpong W, Lee SJ, Ringwald P, Silamut K, Imwong M, Chotivanich K, Lim P, Herdman T, An SS, Yeung S, Singhasivanon P, Day NP, Lindegardh N, Socheat D, White NJ. Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med. 2009;361:455–467. - PMC - PubMed
-
- Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM. Evidence of artemisinin-resistant malaria in western Cambodia. N Engl J Med. 2008;359:2619–2620. - PubMed
-
- Borrmann S, Sasi P, Mwai L, Bashraheil M, Abdallah A, Muriithi S, Fruhauf H, Schaub B, Pfeil J, Peshu J, Hanpithakpong W, Rippert A, Juma E, Tsofa B, Mosobo M, Lowe B, Osier F, Fegan G, Lindegårdh N, Nzila A, Peshu N, Mackinnon M, Marsh K. Declining responsiveness of Plasmodium falciparum infections to artemisinin-based combination treatments on the Kenyan coast. PLoS One. 2011;6:e26005. - PMC - PubMed
-
- Mårtensson A, Stromberg J, Sisowath C, Msellem MI, Gil JP, Montgomery SM, Olliaro P, Ali AS, Björkman A. Efficacy of artesunate plus amodiaquine versus that of artemether-lumefantrine for the treatment of uncomplicated childhood Plasmodium falciparum malaria in Zanzibar, Tanzania. Clin Infect. 2005;41:1079–1086. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
