

Strategies for prevention of postoperative delirium: a systematic review and meta-analysis of randomized trials
- PMID: 23506796
- PMCID: PMC3672487
- DOI: 10.1186/cc12566
Strategies for prevention of postoperative delirium: a systematic review and meta-analysis of randomized trials
Abstract
Introduction: The ideal measures to prevent postoperative delirium remain unestablished. We conducted this systematic review and meta-analysis to clarify the significance of potential interventions.
Methods: The PRISMA statement guidelines were followed. Two researchers searched MEDLINE, EMBASE, CINAHL and the Cochrane Library for articles published in English before August 2012. Additional sources included reference lists from reviews and related articles from 'Google Scholar'. Randomized clinical trials (RCTs) on interventions seeking to prevent postoperative delirium in adult patients were included. Data extraction and methodological quality assessment were performed using predefined data fields and scoring system. Meta-analysis was accomplished for studies that used similar strategies. The primary outcome measure was the incidence of postoperative delirium. We further tested whether interventions effective in preventing postoperative delirium shortened the length of hospital stay.
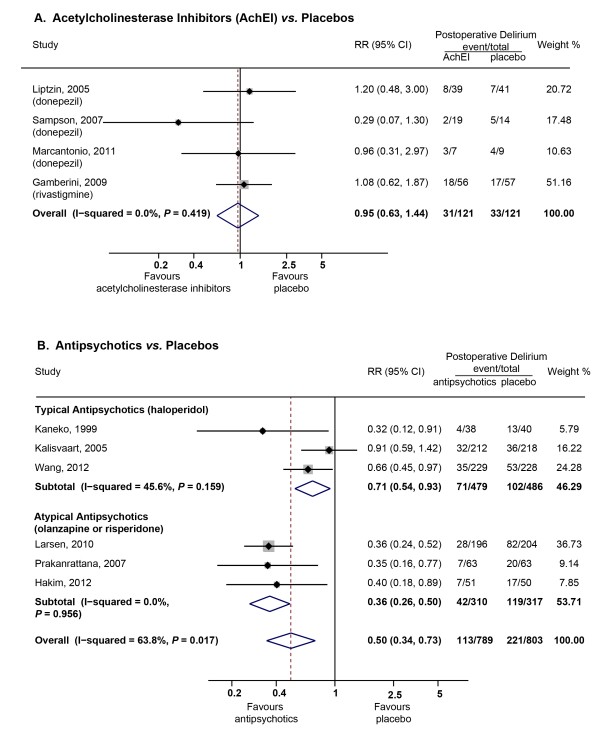
Results: We identified 38 RCTs with interventions ranging from perioperative managements to pharmacological, psychological or multicomponent interventions. Meta-analysis showed dexmedetomidine sedation was associated with less delirium compared to sedation produced by other drugs (two RCTs with 415 patients, pooled risk ratio (RR)=0.39; 95% confidence interval (CI)=0.16 to 0.95). Both typical (three RCTs with 965 patients, RR=0.71; 95% CI=0.54 to 0.93) and atypical antipsychotics (three RCTs with 627 patients, RR=0.36; 95% CI=0.26 to 0.50) decreased delirium occurrence when compared to placebos. Multicomponent interventions (two RCTs with 325 patients, RR=0.71; 95% CI=0.58 to 0.86) were effective in preventing delirium. No difference in the incidences of delirium was found between: neuraxial and general anesthesia (four RCTs with 511 patients, RR=0.99; 95% CI=0.65 to 1.50); epidural and intravenous analgesia (three RCTs with 167 patients, RR=0.93; 95% CI=0.61 to 1.43) or acetylcholinesterase inhibitors and placebo (four RCTs with 242 patients, RR=0.95; 95% CI=0.63 to 1.44). Effective prevention of postoperative delirium did not shorten the length of hospital stay (10 RCTs with 1,636 patients, pooled SMD (standard mean difference)=-0.06; 95% CI=-0.16 to 0.04).
Conclusions: The included studies showed great inconsistencies in definition, incidence, severity and duration of postoperative delirium. Meta-analysis supported dexmedetomidine sedation, multicomponent interventions and antipsychotics were useful in preventing postoperative delirium.
Figures



References
-
- Marcantonio ER, Goldman L, Mangione CM, Ludwig LE, Muraca B, Haslauer CM, Donaldson MC, Whittemore AD, Sugarbaker DJ, Poss R, Hass S, Cook EF, Orav EJ, Lee TH. A clinical prediction rule for delirium after elective noncardiac surgery. JAMA. 1994;271:134–139. doi: 10.1001/jama.1994.03510260066030. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
