

The synergistic relationship between estimated GFR and microalbuminuria in predicting long-term progression to ESRD or death in patients with diabetes: results from the Kidney Early Evaluation Program (KEEP)
- PMID: 23507266
- PMCID: PMC4492431
- DOI: 10.1053/j.ajkd.2013.01.005
The synergistic relationship between estimated GFR and microalbuminuria in predicting long-term progression to ESRD or death in patients with diabetes: results from the Kidney Early Evaluation Program (KEEP)
Abstract
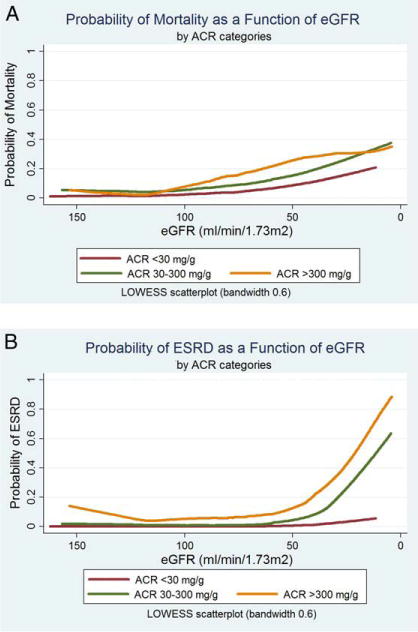
Introduction: Chronic kidney disease may complicate diabetes, often manifesting with reduced glomerular filtration rate (GFR), albuminuria, or both. Although greater albuminuria and lower estimated GFR both predict adverse prognosis, whether a synergistic prognostic interaction occurs in patients with diabetes has not been defined in a large national cohort study.
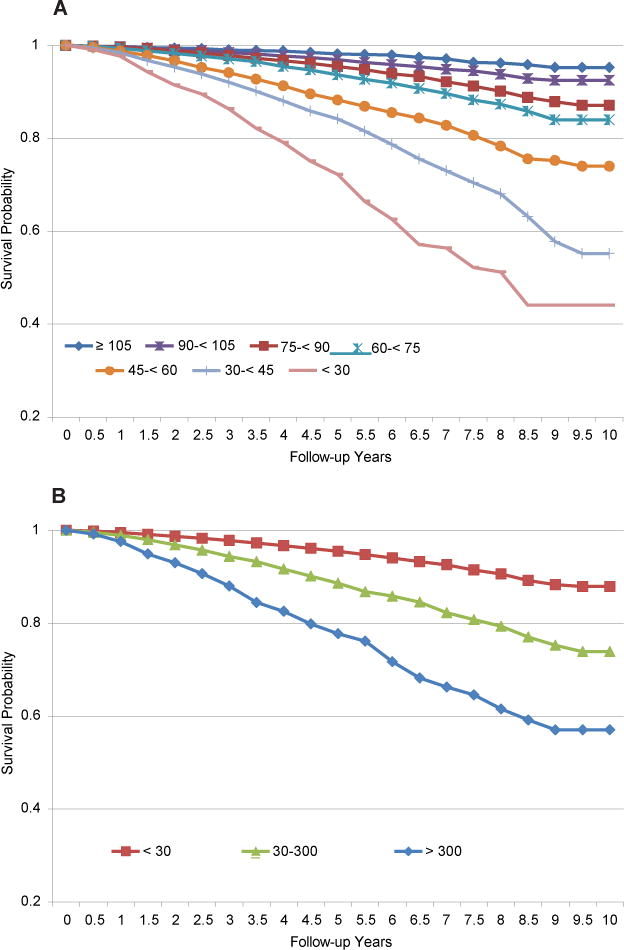
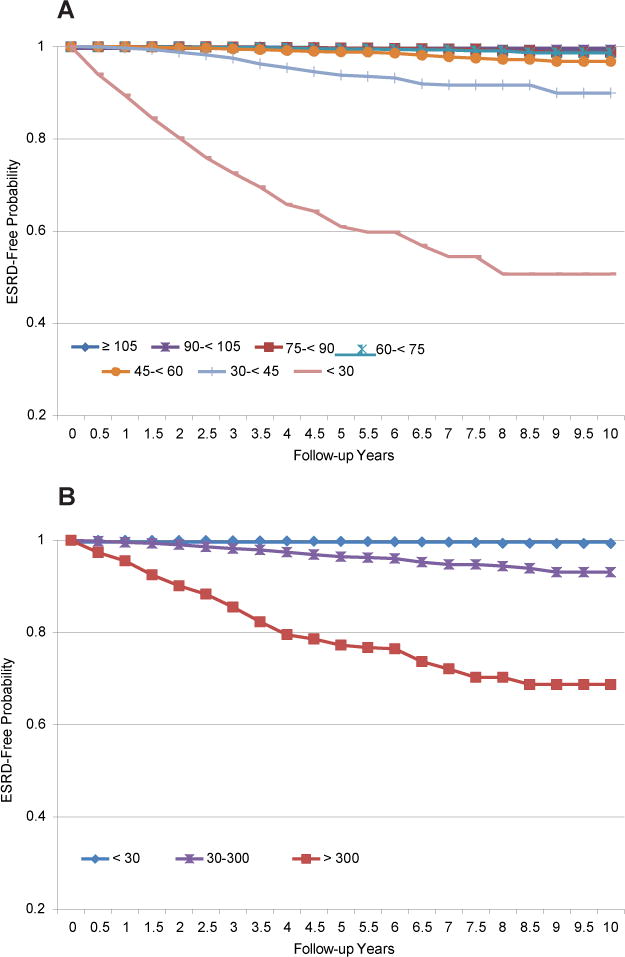
Methods: We used 2000-2011 data from the National Kidney Foundation's Kidney Early Evaluation Program (KEEP) for 42,761 participants with diabetes. Kaplan-Meier survival analysis and multivariable Cox regression were used to ascertain the association of estimated GFR, albumin-creatinine ratio (ACR), and their interaction on all-cause mortality and progression to end-stage renal disease (ESRD) at a median 4 years of follow-up.
Results: Of 42,761 participants with diabetes, 8,618 (20.2%) had estimated GFR <60 mL/min/1.73 m(2), 7,715 (18.0%) had ACR >30 mg/g, and 2,641 (6.2%) had both. The unadjusted incidence (per 1,000 person-years) of all-cause mortality increased from 3.1 (95% CI, 2.4-3.8) in participants with estimated GFR ≥ 105 mL/min/1.73 m(2) and no albuminuria to 73.7 (95% CI, 54.9-92.5) in participants with estimated GFR <30 mL/min/1.73 m(2) and macroalbuminuria (P < 0.001). Progression to ESRD likewise increased from 0.2 (95% CI, 0-0.4) to 220.4 (95% CI, 177.2-263.6) per 1,000 person-years (P < 0.001). After adjustment for confounders, both estimated GFR and albuminuria were associated independently with mortality and progression to ESRD, with a strong synergistic interaction (P for interaction < 0.001); estimated GFR <30 mL/min/1.73 m(2) and macroalbuminuria together were associated with a 5-fold higher risk of mortality and a more than 1,000-fold higher risk of progression to ESRD (compared with patients with estimated GFR >60 mL/min/1.73 m(2) and ACR <30 mg/g; P < 0.001 for both outcomes).
Conclusions: In this large cohort of diabetic KEEP participants with more than 170,000 person-years of follow-up, both estimated GFR and albuminuria were associated independently with mortality and progression to ESRD, with a strong synergistic interaction.
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Vora JP, Ibrahim HA, Bakris GL. Responding to the challenge of diabetic nephropathy: the historic evolution of detection, prevention and management. J Hum Hypertens. 2000;14(10–11):667–685. - PubMed
-
- Dronavalli S, Duka I, Bakris GL. The pathogenesis of diabetic nephropathy. Nat Clin Pract Endocrinol Metab. 2008;4(8):444–452. - PubMed
-
- Soldatos G, Cooper ME. Diabetic nephropathy: important pathophysiologic mechanisms. Diabetes Res Clin Pract. 2008;82(suppl 1):S75–S79. - PubMed
-
- Penno G, Solini A, Bonora E, et al. Clinical significance of nonalbuminuric renal impairment in type 2 diabetes. J Hypertens. 2011;29(9):1802–1809. - PubMed
-
- Macisaac RJ, Tsalamandris C, Panagiotopoulos S, Smith TJ, McNeil KJ, Jerums G. Nonalbuminuric renal insufficiency in type 2 diabetes. Diabetes Care. 2004;27(1):195–200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
