

AO spine injury classification system: a revision proposal for the thoracic and lumbar spine
- PMID: 23508335
- PMCID: PMC3804719
- DOI: 10.1007/s00586-013-2738-0
AO spine injury classification system: a revision proposal for the thoracic and lumbar spine
Abstract
Purpose: The AO Spine Classification Group was established to propose a revised AO spine injury classification system. This paper provides details on the rationale, methodology, and results of the initial stage of the revision process for injuries of the thoracic and lumbar (TL) spine.
Methods: In a structured, iterative process involving five experienced spine trauma surgeons from various parts of the world, consecutive cases with TL injuries were classified independently by members of the classification group, and analyzed for classification reliability using the Kappa coefficient (κ) and for accuracy using latent class analysis. The reasons for disagreements were examined systematically during review meetings. In four successive sessions, the system was revised until consensus and sufficient reproducibility were achieved.
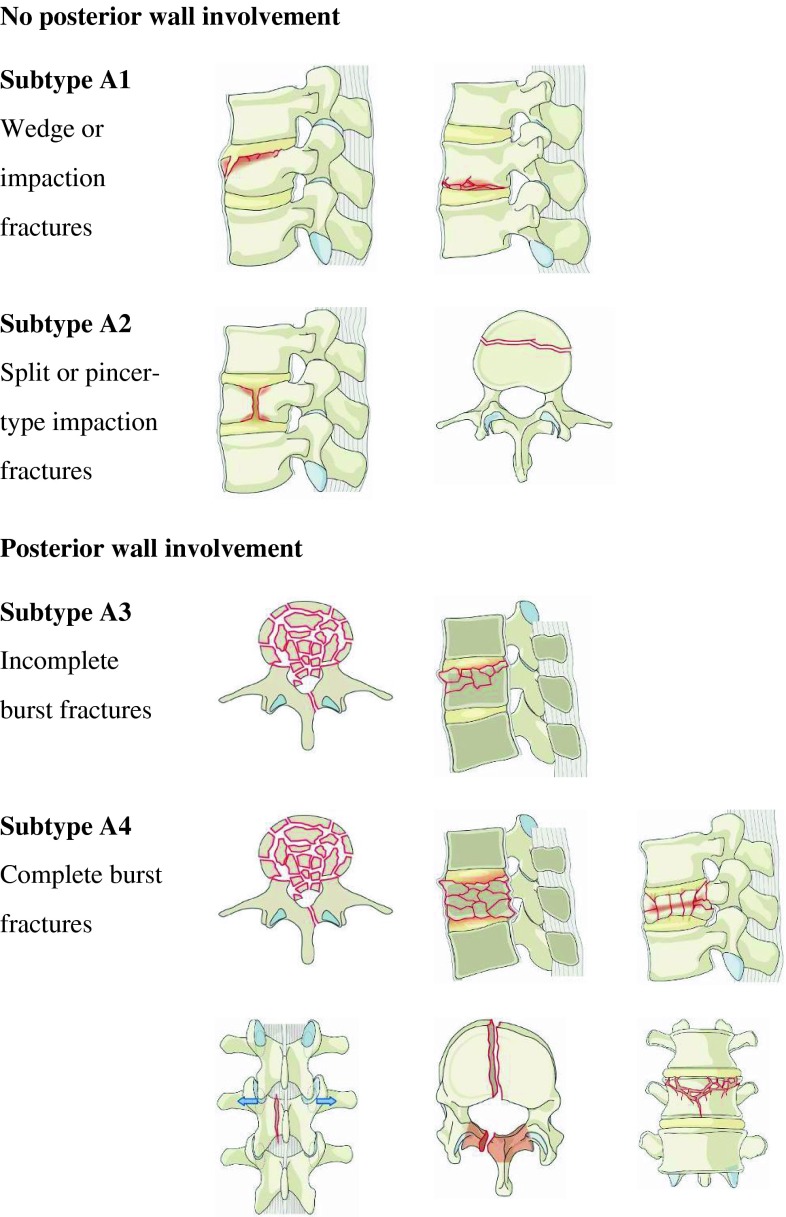
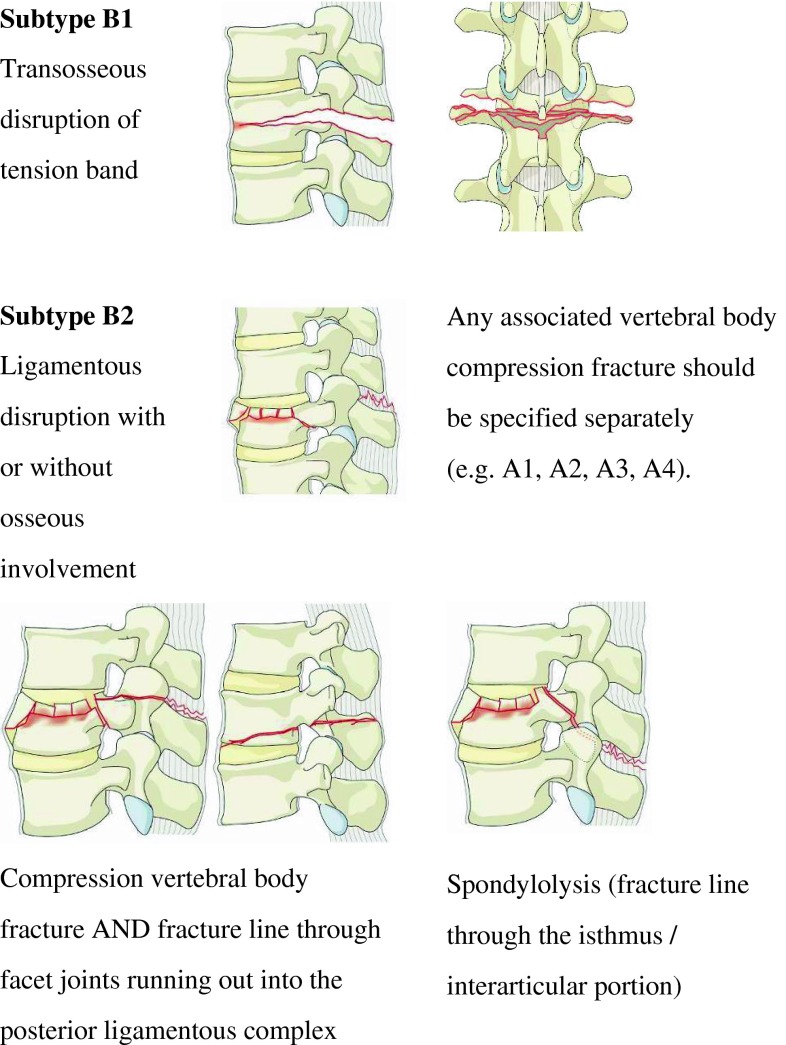
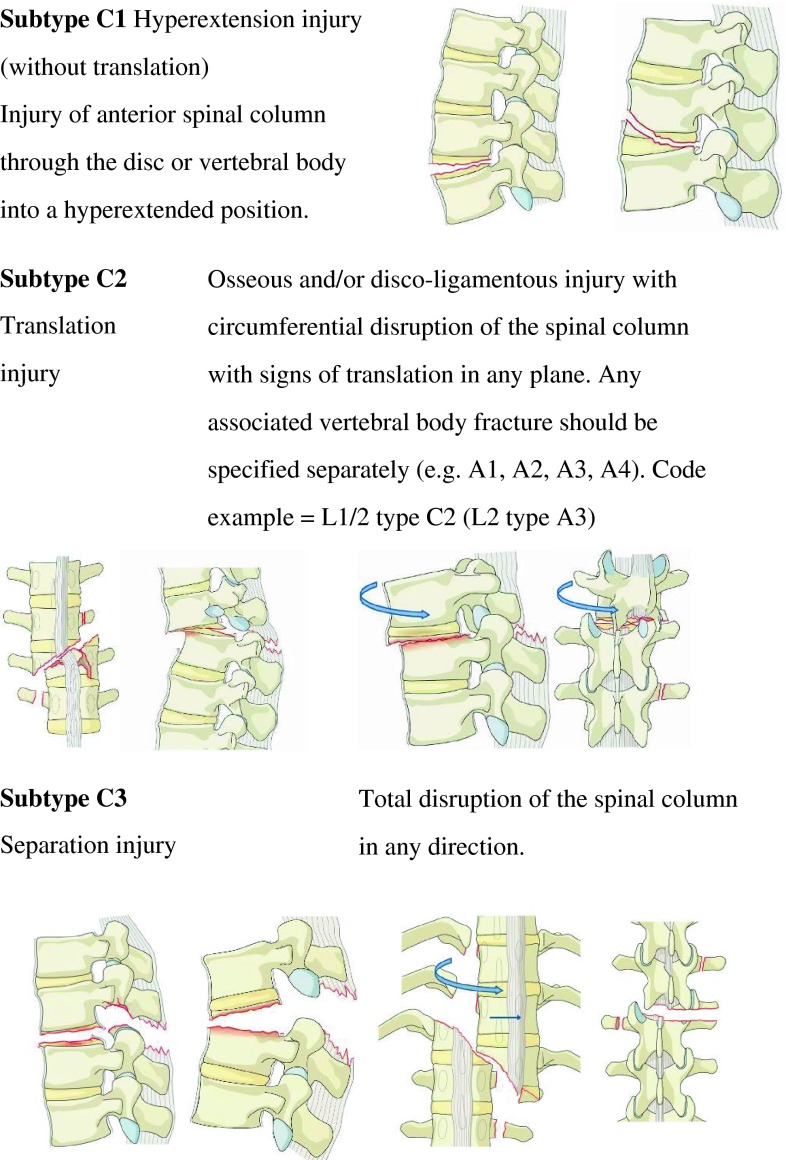
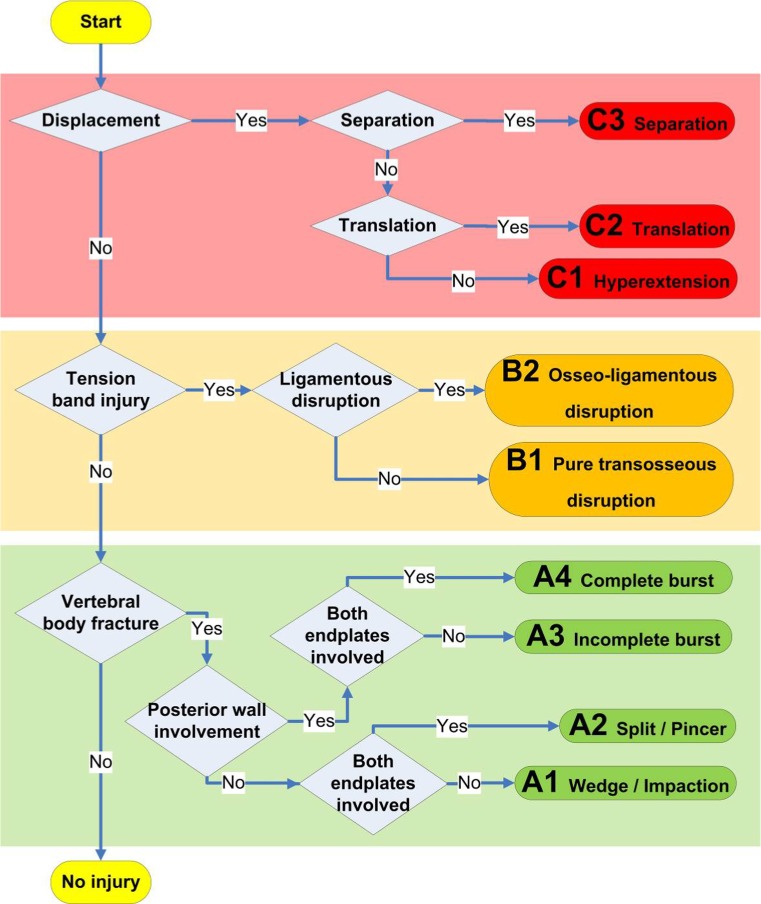
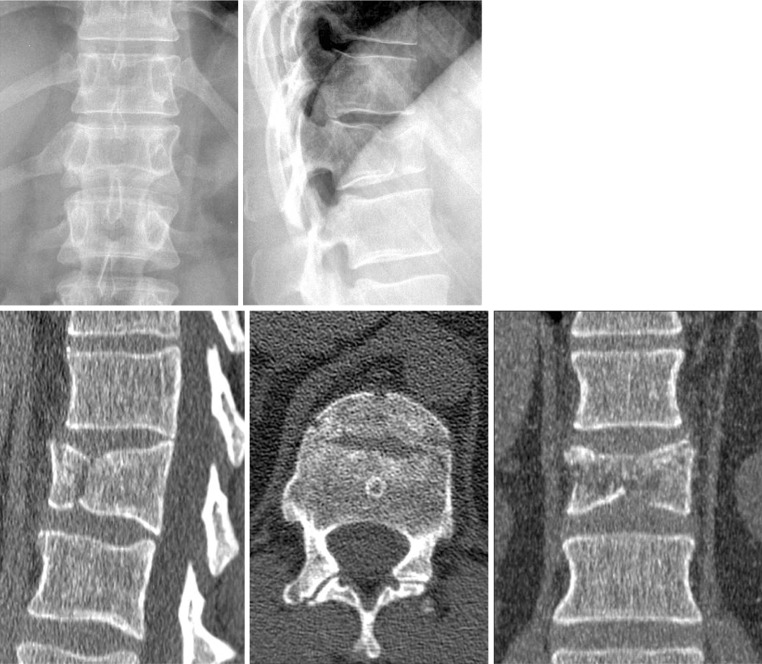
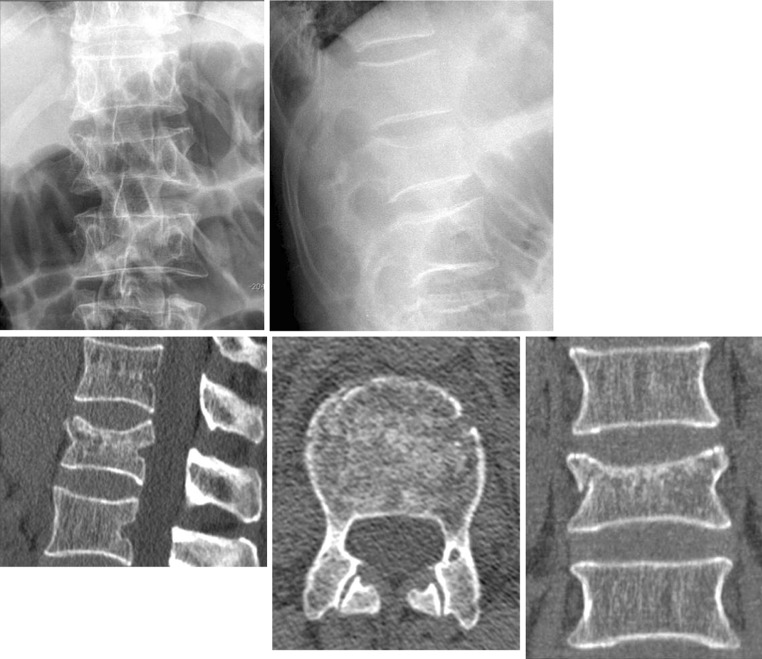
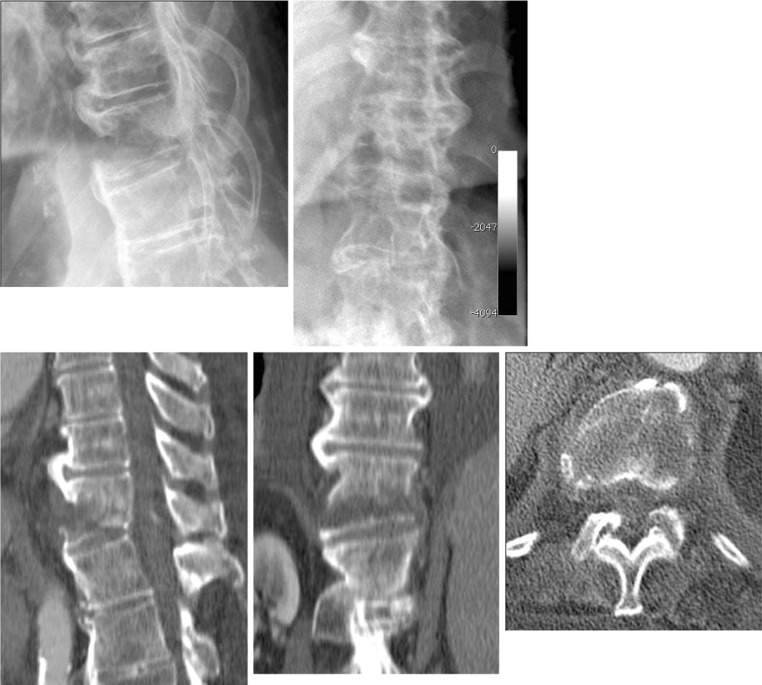
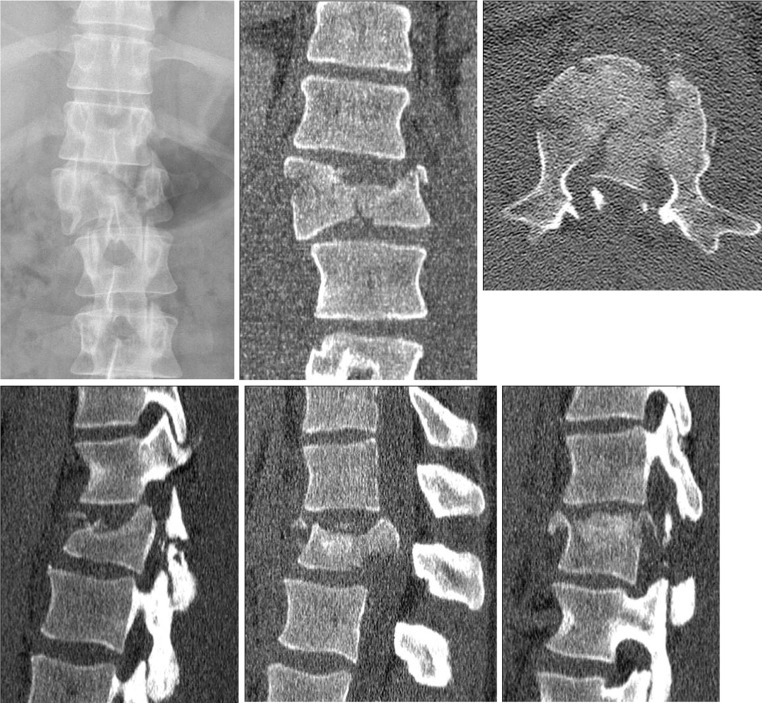
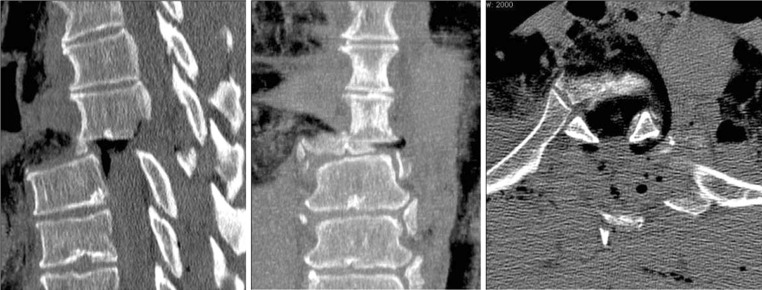
Results: The TL spine injury system is based on three main injury categories adapted from the original Magerl AO concept: A (compression), B (tension band), and C (displacement) type injuries. Type-A injuries include four subtypes (wedge-impaction/split-pincer/incomplete burst/complete burst); B-type injuries are divided between purely osseous and osseo-ligamentous disruptions; and C-type injuries are further categorized into three subtypes (hyperextension/translation/separation). There is no subgroup division. The reliability of injury types (A, B, C) was good (κ = 0.77). The surgeons' pairwise Kappa ranged from 0.69 to 0.90. Kappa coefficients κ for reliability of injury subtypes ranged from 0.26 to 0.78.
Conclusions: The proposed TL spine injury system is based on clinically relevant parameters. Final evaluation data showed reasonable reliability and accuracy. Further validation of the proposed revised AO Classification requires follow-up evaluation sessions and documentation by more surgeons from different countries and backgrounds and is subject to modification based on clinical parameters during subsequent phases.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
