

Operative Management of a Sacral Gunshot Injury via Minimally Invasive Techniques and Instrumentation
- PMID: 23508557
- PMCID: PMC3596584
- DOI: 10.4184/asj.2013.7.1.44
Operative Management of a Sacral Gunshot Injury via Minimally Invasive Techniques and Instrumentation
Abstract
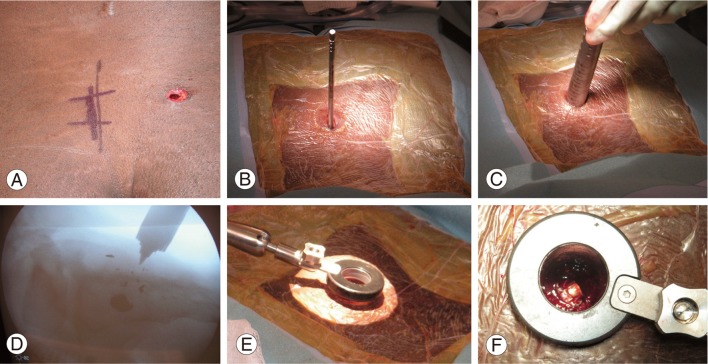
Gunshot wounds to the spine account for 13% to 17% of all gunshot injuries and occur predominantly in the thoracic region. Minimally invasive spine surgery procedures implementing serial muscle dilation and the use of a tubular retracting system with a working channel minimize soft tissue trauma, facilitate less bony and soft tissue resection, decrease blood loss, minimize scarring and improve cosmesis, decrease hospitalization, and reduce postoperative pain and narcotic usage in comparison to more open, traditional approaches. Although minimally invasive spine surgery techniques and instrumentation have gained considerable attention, their application in the management of gunshot injuries to the sacrum has not been reported. The following is a brief case report of a 21-year-old male who sustained a gunshot injury to the sacrum who was managed operatively via minimally invasive spine surgery techniques and instrumentation.
Keywords: Gunshot wound; Minimally invasive; Sacral; Spine; Surgery; Trauma.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures



Similar articles
-
Minimally Invasive Management of Civilian Gunshot Wounds to the Lumbar Spine: A Case Series and Technical Report.Oper Neurosurg. 2020 Sep 1;19(3):219-225. doi: 10.1093/ons/opaa030. Oper Neurosurg. 2020. PMID: 32147736
-
[Precise application of Traditional Chinese Medicine in minimally-invasive techniques].Zhongguo Gu Shang. 2018 Jun 25;31(6):493-496. doi: 10.3969/j.issn.1003-0034.2018.06.001. Zhongguo Gu Shang. 2018. PMID: 29945400 Chinese.
-
Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma.Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Neurosurg Focus. 2014. PMID: 24981899 Review.
-
Minimally Invasive Muscle Sparing Posterior-Only Approach for Lumbar Circumferential Decompression and Stabilization to Treat Spine Metastasis--Technical Report.World Neurosurg. 2015 Nov;84(5):1484-90. doi: 10.1016/j.wneu.2015.06.018. Epub 2015 Jun 20. World Neurosurg. 2015. PMID: 26100166
-
The use of minimally invasive surgery in spine trauma: a review of concepts.J Spine Surg. 2019 Jun;5(Suppl 1):S91-S100. doi: 10.21037/jss.2019.04.13. J Spine Surg. 2019. PMID: 31380497 Free PMC article. Review.
Cited by
-
Case Report: Full-Endoscopic Surgery for Bullet Wounds of the Spine: A Report of Three Cases.Front Surg. 2022 Mar 25;9:873365. doi: 10.3389/fsurg.2022.873365. eCollection 2022. Front Surg. 2022. PMID: 35402482 Free PMC article.
-
Management of a posterior gunshot injury with a floating pedicle and cerebrospinal fluid leak.Eur Spine J. 2018 Aug;27(8):1681-1687. doi: 10.1007/s00586-018-5537-9. Epub 2018 Mar 10. Eur Spine J. 2018. PMID: 29525911 Review.
-
Current concepts in penetrating and blast injury to the central nervous system.World J Surg. 2015 Jun;39(6):1352-62. doi: 10.1007/s00268-014-2874-7. World J Surg. 2015. PMID: 25446474 Free PMC article. Review.
-
Operative Intervention for Lumbar Foraminal Gunshot Wounds: Case Report and Review of the Literature.Cureus. 2019 Jul 29;11(7):e5269. doi: 10.7759/cureus.5269. Cureus. 2019. PMID: 31576262 Free PMC article.
References
-
- Aryan HE, Amar AP, Ozgur BM, Levy ML. Gunshot wounds to the spine in adolescents. Neurosurgery. 2005;57:748–752. - PubMed
-
- Farmer JC, Vaccaro AR, Balderston RA, Albert TJ, Cotler J. The changing nature of admissions to a spinal cord injury center: violence on the rise. J Spinal Disord. 1998;11:400–403. - PubMed
-
- Kupcha PC, An HS, Cotler JM. Gunshot wounds to the cervical spine. Spine. 1990;15:1058–1063. - PubMed
-
- Anderson DG, Samartzis D, Shen FH, Tannoury C. Percutaneous instrumentation of the thoracic and lumbar spine. Orthop Clin North Am. 2007;38:401–408. - PubMed
-
- Perez-Cruet MJ, Wang MY, Samartzis D. Microendoscopic cervical laminoplasty and laminectomy. In: Kim DH, Fessler RG, Regan JJ, editors. Endoscopic spine surgery and instrumentation. New York: Thieme; 2005. pp. 74–87.
LinkOut - more resources
Full Text Sources
Other Literature Sources
