

Risks and benefits associated with antibiotic use for acute respiratory infections: a cohort study
- PMID: 23508604
- PMCID: PMC3601395
- DOI: 10.1370/afm.1449
Risks and benefits associated with antibiotic use for acute respiratory infections: a cohort study
Abstract
Purpose: Antibiotics are frequently prescribed for acute nonspecific respiratory infections (ARIs), presumably to avoid small risks of progression to serious bacterial illness. However, even low risks of associated adverse drug events could result in many such events at the population level. Our objective was to assess the risks and benefits of antibiotic use in a cohort of patients with ARIs, comparing outcomes of patients who were prescribed antibiotics with outcomes of patients not receiving antibiotics.
Methods: We used a June 1986 to August 2006 cohort of adult patients with ARI visits from a UK primary care database. Exposure was an antibiotic prescribed with the visit. Primary outcomes were hospitalization within 15 days for (1) severe adverse drug events (hypersensitivity, diarrhea, seizure, arrhythmia, hepatic or renal failure), and (2) community-acquired pneumonia.
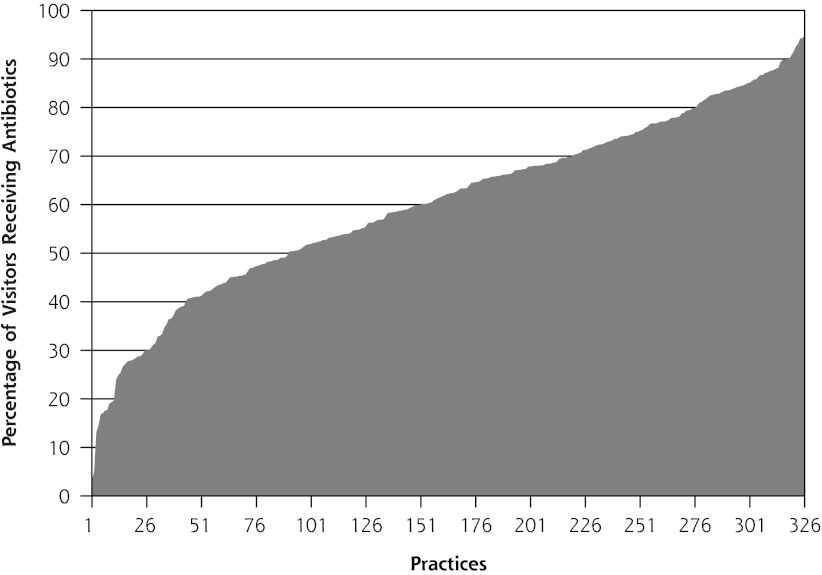
Results: The cohort included 1,531,019 visits with an ARI diagnosis; prescriptions for antibiotics were given in 65% of cases. The adjusted risk difference for treated vs untreated patients per 100,000 visits was 1.07 fewer adverse events (95% CI, -4.52 to 2.38; P = .54) and 8.16 fewer pneumonia hospitalizations (95% CI, -13.24 to -3.08; P = .002). The number needed to treat to prevent 1 hospitalization for pneumonia was 12,255.
Conclusions: Compared with patients with ARI who were not treated with antibiotics, patients who were treated with antibiotics were not at increased risk of severe adverse drug events and had a small decreased risk of pneumonia hospitalization. This small benefit from antibiotics for a common ambulatory diagnosis creates persistent tension; at the societal level, physicians are compelled to reduce antibiotic prescribing, thus minimizing future resistance, whereas at the encounter level, they are compelled to optimize the benefit-risk balance for that patient.
Figures
References
-
- Col NF, O’Connor RW. Estimating worldwide current antibiotic usage: report of Task Force 1. Rev Infect Dis. 1987;9(Suppl 3):S232–S243 - PubMed
-
- Halasa NB, Griffin MR, Zhu Y, Edwards KM. Decreased number of antibiotic prescriptions in office-based settings from 1993 to 1999 in children less than five years of age. Pediatr Infect Dis J. 2002;21(11):1023–1028 - PubMed
-
- Finkelstein JA, Stille C, Nordin J, et al. Reduction in antibiotic use among US children, 1996–2000. Pediatrics. 2003;112(3 Pt 1):620–627 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical