

Locking-plate osteosynthesis versus intramedullary nailing for fixation of olecranon fractures: a biomechanical study
- PMID: 23508868
- PMCID: PMC3631502
- DOI: 10.1007/s00264-013-1854-0
Locking-plate osteosynthesis versus intramedullary nailing for fixation of olecranon fractures: a biomechanical study
Abstract
Purpose: Intramedullary nailing and locked plating for fixation of olecranon fractures has recently gained popularity. However, these two new technologies have not been compared for their biomechanical efficacy. The aim of this study was to evaluate the biomechanical stability of two newly designed fracture fixation devices for treating olecranon fractures during dynamic continuous loading: the ION intramedullary locking nail and the LCP precontoured locking compression plate.
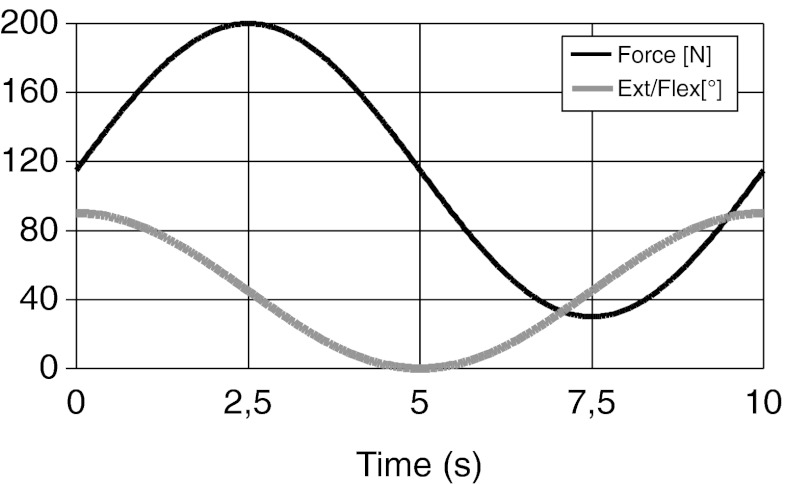
Methods: Simulated oblique olecranon fractures were created in eight pairs of fresh-frozen cadaver ulnae and stabilised using either the LCP or ION. Specimens were then subjected to continuous dynamic loading (from 25 to 200 N), with a continuous angle alteration between 0° and 90° of flexion, to perform a matched-pairs comparison. Significant differences in the distance between markers surrounding the fracture gap was determined using the Wilcoxon test after four and 300 loading cycles.
Results: The ION resulted in significantly less displacement in the fracture gap at 0° extension (P = 0.036), 45° flexion (P = 0.035) and 90° flexion (P = 0.017) after 300 cycles of continuous loading. The measured displacements were small and were probably not of clinical significance. No mechanical failure or hardware migration was seen with either fixation technique.
Conclusion: This study shows significantly less micromotion for the ION than for the LCP in treating oblique olecranon fractures after 300 cycles of dynamic loading. Both implant types could be appropriate surgical techniques for fixation of selected olecranon fractures and osteotomies.
Figures




References
-
- Macko D, Szabo RM. Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am. 1985;67:1396–1401. - PubMed
-
- Murphy DF, Greene WB, Dameron TB Jr (1987) Displaced olecranon fractures in adults. Clinical evaluation. Clin Orthop Relat Res 215–223 - PubMed
-
- Hume MC, Wiss DA (1992) Olecranon fractures. A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 229–235 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
