

Three-gene immunohistochemical panel adds to clinical staging algorithms to predict prognosis for patients with esophageal adenocarcinoma
- PMID: 23509313
- PMCID: PMC3625712
- DOI: 10.1200/JCO.2012.45.9636
Three-gene immunohistochemical panel adds to clinical staging algorithms to predict prognosis for patients with esophageal adenocarcinoma
Abstract
Purpose: Esophageal adenocarcinoma (EAC) is a highly aggressive disease with poor long-term survival. Despite growing knowledge of its biology, no molecular biomarkers are currently used in routine clinical practice to determine prognosis or aid clinical decision making. Hence, this study set out to identify and validate a small, clinically applicable immunohistochemistry (IHC) panel for prognostication in patients with EAC.
Patients and methods: We recently identified eight molecular prognostic biomarkers using two different genomic platforms. IHC scores of these biomarkers from a UK multicenter cohort (N = 374) were used in univariate Cox regression analysis to determine the smallest biomarker panel with the greatest prognostic power with potential therapeutic relevance. This new panel was validated in two independent cohorts of patients with EAC who had undergone curative esophagectomy from the United States and Europe (N = 666).
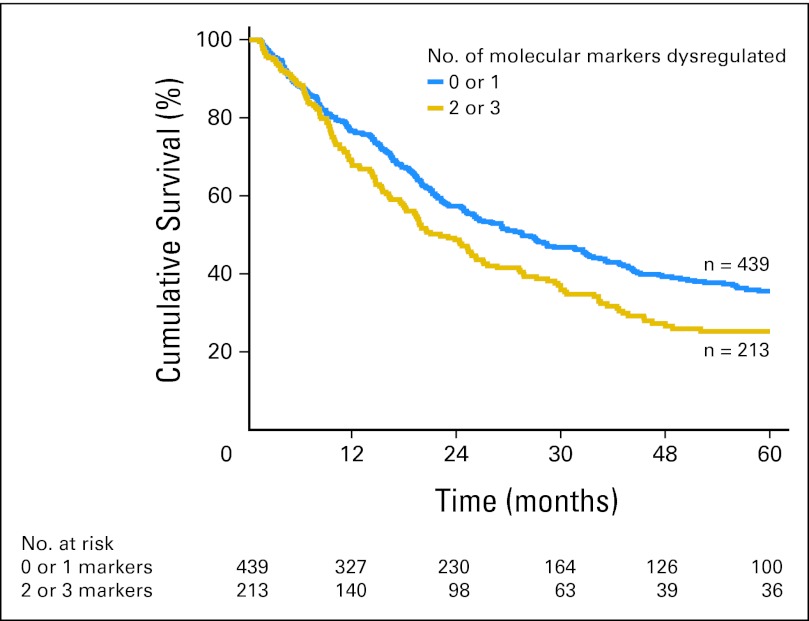
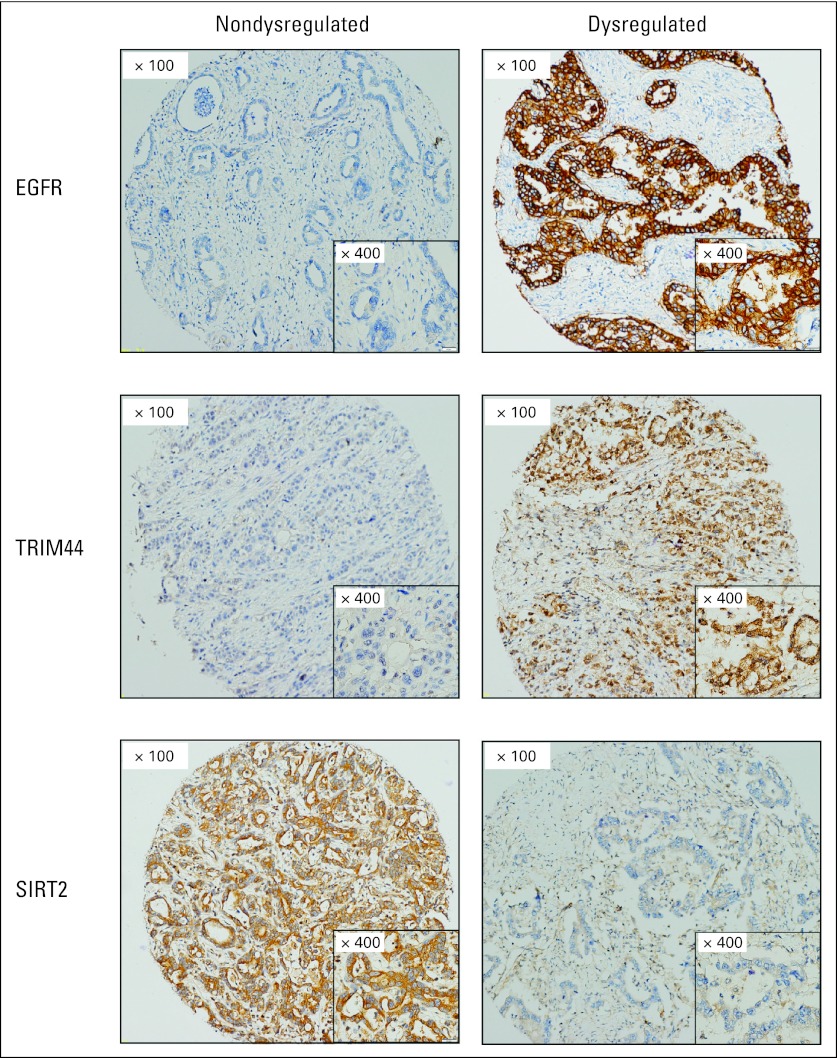
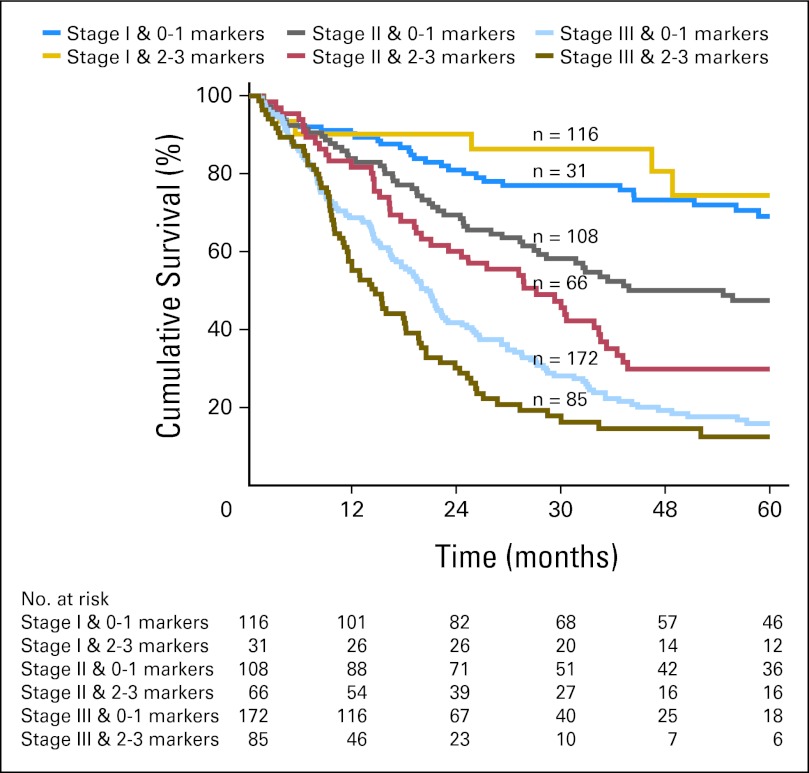
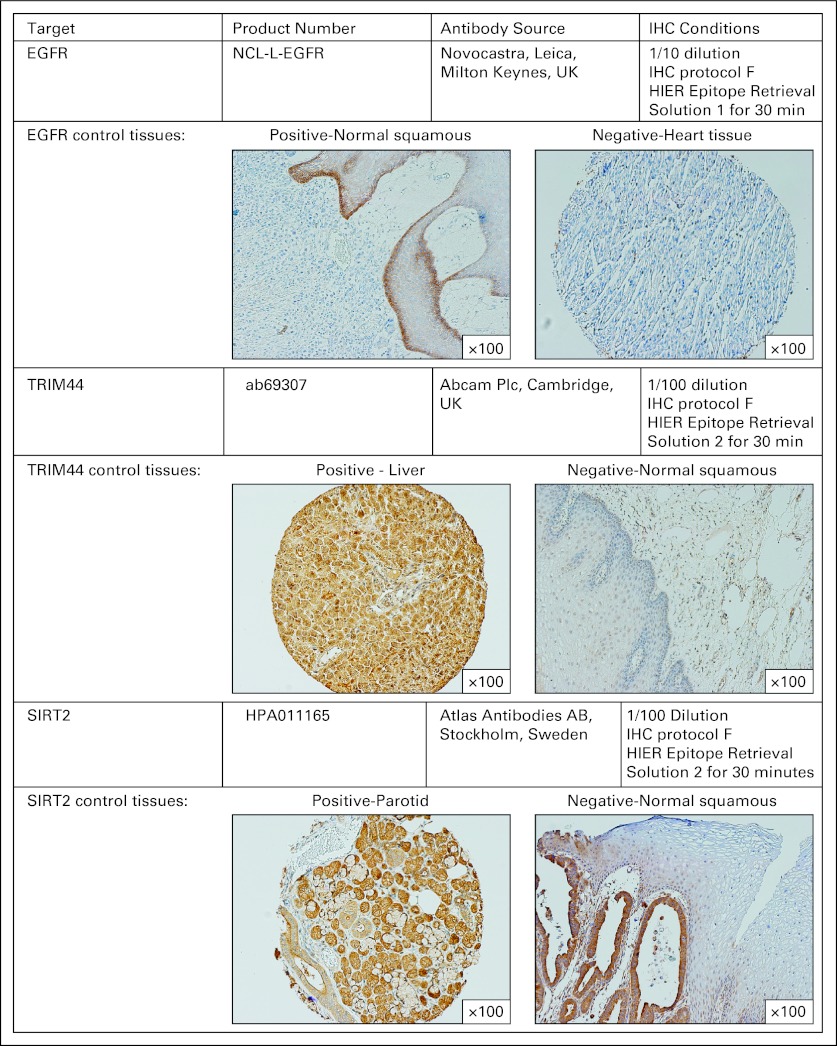
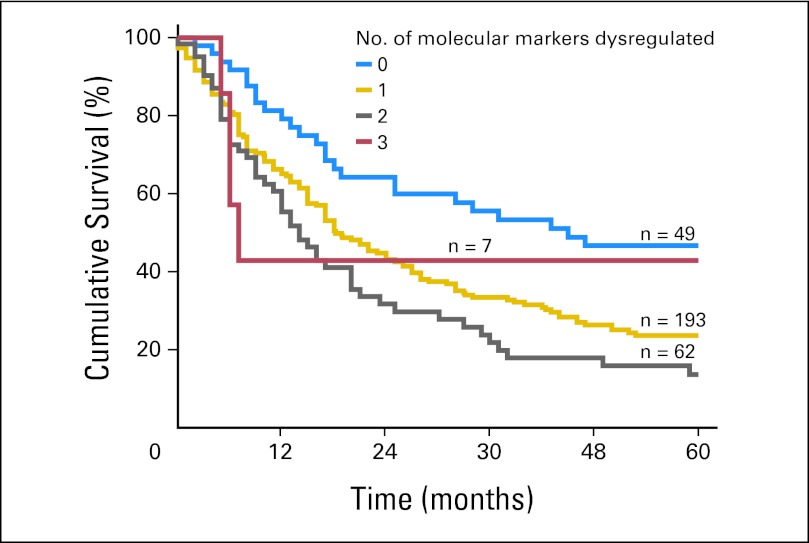
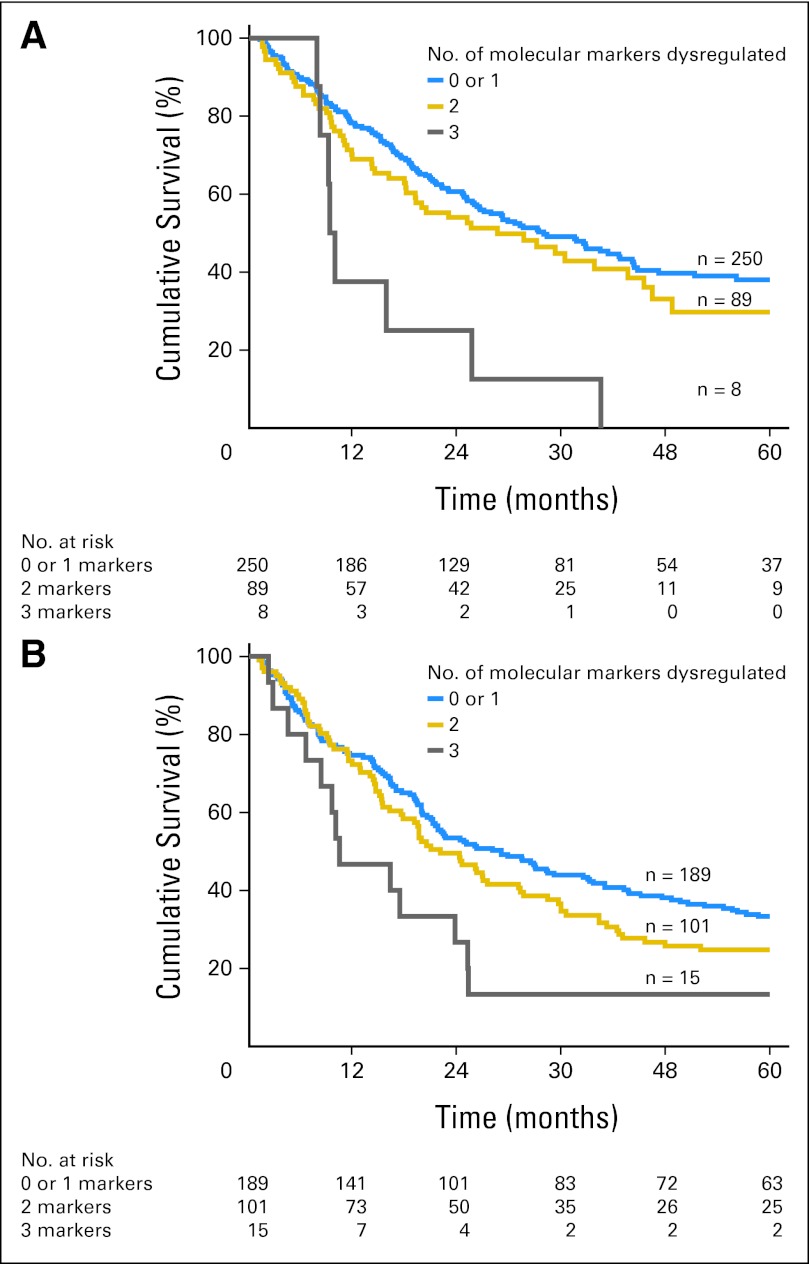
Results: Three of the eight previously identified prognostic molecular biomarkers (epidermal growth factor receptor [EGFR], tripartite motif-containing 44 [TRIM44], and sirtuin 2 [SIRT2]) had the strongest correlation with long-term survival in patients with EAC. Applying these three biomarkers as an IHC panel to the validation cohort segregated patients into two different prognostic groups (P < .01). Adjusting for known survival covariates, including clinical staging criteria, the IHC panel remained an independent predictor, with incremental adverse overall survival (OS) for each positive biomarker (hazard ratio, 1.20; 95% CI, 1.03 to 1.40 per biomarker; P = .02).
Conclusion: We identified and validated a clinically applicable IHC biomarker panel, consisting of EGFR, TRIM44, and SIRT2, that is independently associated with OS and provides additional prognostic information to current survival predictors such as stage.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Pohl H, Sirovich B, Welch HG. Esophageal adenocarcinoma incidence: Are we reaching the peak? Cancer Epidemiol Biomarkers Prev. 2010;19:1468–1470. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Edge SB, Byrd DR, Compton CC, et al. New York, NY: Springer; 2010. AJCC Cancer Staging Manual (ed 7)
-
- Johansson J, DeMeester TR, Hagen JA, et al. En bloc vs transhiatal esophagectomy for stage T3 N1 adenocarcinoma of the distal esophagus. Arch Surg. 2004;139:627–631. discussion 631-633. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
