

Thirteen Years of Hyoid Suspension Experience in Multilevel OSAHS Surgery: The Short-Term Results of a Bicentric Study
- PMID: 23509464
- PMCID: PMC3590780
- DOI: 10.1155/2013/263043
Thirteen Years of Hyoid Suspension Experience in Multilevel OSAHS Surgery: The Short-Term Results of a Bicentric Study
Abstract
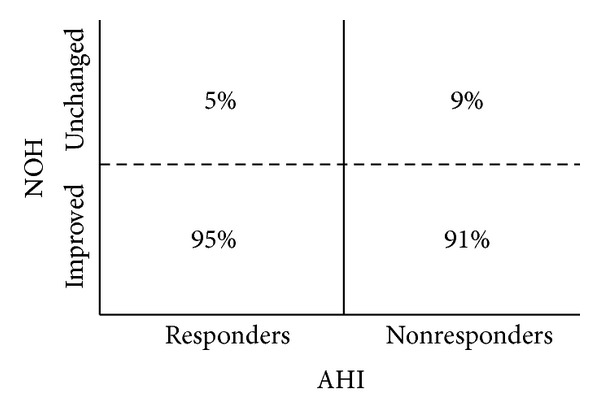
Aims. To evaluate thirteen years of hyoid suspension experience in multilevel OSAHS surgery, for which hyoidthyroidpexia represented the exclusive hypopharyngeal approach applied. Materials and Methods. From 1998 to 2011, a bicentric retrospective study was conducted: all adult patients with a diagnosis of OSAHS were enrolled. Specific eligible criteria were established. Pre-/postoperative data concerning ENT and sleep findings were recorded. Recruited subjects were surveilled for a follow-up range from 6 to 18 months. Results. A total of 590 hyoid suspensions were evaluated, but only 140 patients met the specific inclusion criteria. A success rate of 67% was obtained. No intraoperative adverse events or major complications occurred. Excessive daytime sleepiness was observed in 28% of nonresponders. Despite the homogeneous candidate anatomy, ENT awake findings changed differently after surgery. Statistical analysis revealed multilevel surgery to be more effective when AHI < 30. Postoperative AHI was statistically not influenced by preoperative BMI. Conclusions. Hyoid suspension in multilevel treatment is effective when short-term results are considered. The necessity of a more valuable anatomic-based diagnostic approach is crucial to guide the patient selection. Long-term followups and randomized prospective trials with case-control series are needed to increase the level of evidence of this surgery.
Figures



Similar articles
-
The effect of hyoid suspension in a multilevel surgery concept for obstructive sleep apnea.Otolaryngol Head Neck Surg. 2006 May;134(5):856-61. doi: 10.1016/j.otohns.2006.01.015. Otolaryngol Head Neck Surg. 2006. PMID: 16647548
-
Combined elliptical window genioglossus advancement, hyoid bone suspension, and uvulopalatopharyngoplasty decrease apnea hypopnea index and subjective daytime sleepiness in obstructive sleep apnea.J Oral Maxillofac Surg. 2013 Oct;71(10):1729-32. doi: 10.1016/j.joms.2013.06.001. Epub 2013 Aug 8. J Oral Maxillofac Surg. 2013. PMID: 23932115
-
Hyoidthyroidpexia as a treatment in multilevel surgery for obstructive sleep apnea.Acta Otolaryngol. 2008 Jun;128(6):680-4. doi: 10.1080/00016480701636884. Acta Otolaryngol. 2008. PMID: 18568505
-
Hyoid Bone Suspension as a Part of Multilevel Surgery for Obstructive Sleep Apnea Syndrome.Int Arch Otorhinolaryngol. 2018 Jul;22(3):266-270. doi: 10.1055/s-0037-1607227. Epub 2017 Oct 25. Int Arch Otorhinolaryngol. 2018. PMID: 29983767 Free PMC article.
-
Obstructive sleep apnea/hypopnea syndrome.Panminerva Med. 2013 Jun;55(2):191-5. Panminerva Med. 2013. PMID: 23676959 Review.
Cited by
-
Oromaxillofacial Surgery: Both a Treatment and a Possible Cause of Obstructive Sleep Apnea-A Narrative Review.Life (Basel). 2023 Jan 4;13(1):142. doi: 10.3390/life13010142. Life (Basel). 2023. PMID: 36676088 Free PMC article. Review.
-
Sleepiness Score-Specific Outcomes of a Novel Tongue Repositioning Procedure for the Treatment of Continuous Positive Airway Pressure-Resistant Obstructive Sleep Apnea.Ann Maxillofac Surg. 2019 Jan-Jun;9(1):28-36. doi: 10.4103/ams.ams_151_18. Ann Maxillofac Surg. 2019. PMID: 31293927 Free PMC article.
References
-
- Kuhlo W, Doll E, Franck MC. Successful management of Pickwickian syndrome using long-term tracheostomy. Deutsche Medizinische Wochenschrift. 1969;94(24):1286–1290. - PubMed
-
- Vicini C, Dallan I, Canzi P, Frassineti S, La Pietra MG, Montevecchi F. Transoral robotic tongue base resection in obstructive sleep apnoea-hypopnoea syndrome: a preliminary report. ORL Journal of Otorhinolaryngology and Its Related Specialties. 2010;72(1):22–27. - PubMed
-
- Sher AE, Schechtman KB, Piccirillo JF. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep. 1996;19(2):156–177. - PubMed
-
- Riley RW, Powell NB, Guilleminault C. Inferior sagittal osteotomy of the mandible with hyoid myotomy-suspension: a new procedure for obstructive sleep apnea. Otolaryngology. 1986;94(5):589–593. - PubMed
-
- Patton TJ, Thawley SE, Water RC, Vandermeer PJ, Ogura JH. Expansion hyoidplasty: a potential surgical procedure designed for selected patients with obstructive sleep apnea syndrome. Experimental canine results. Laryngoscope. 1983;93(11 I):1387–1396. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
