

Dissecting graft-versus-leukemia from graft-versus-host-disease using novel strategies
- PMID: 23510414
- PMCID: PMC3645301
- DOI: 10.1111/tan.12090
Dissecting graft-versus-leukemia from graft-versus-host-disease using novel strategies
Abstract
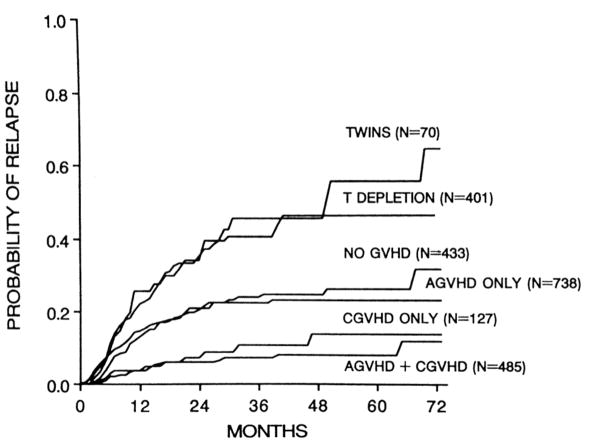
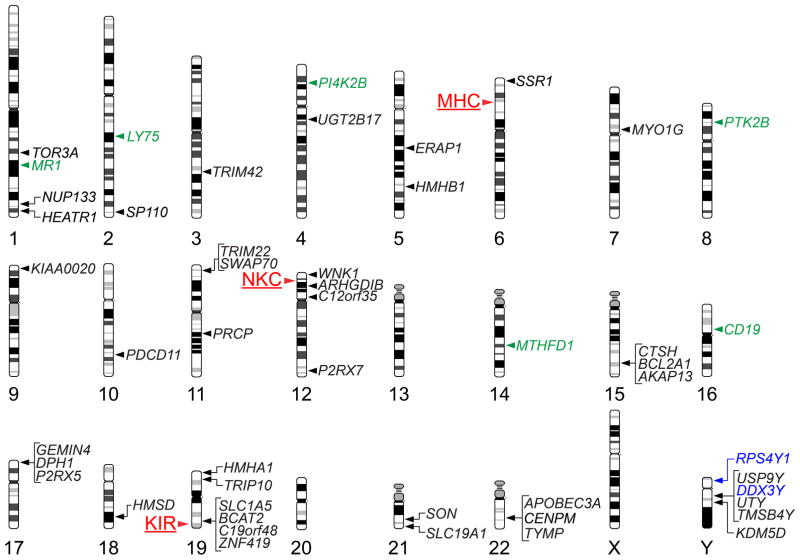
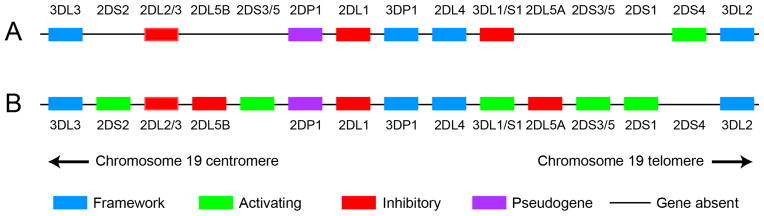
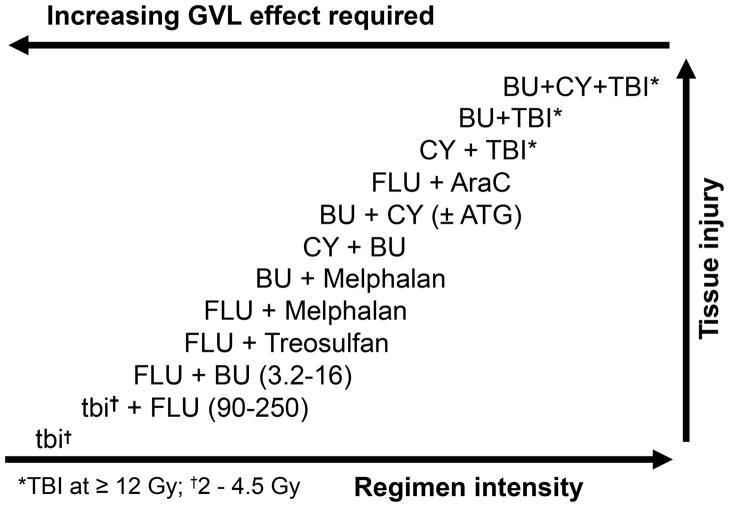
The intrinsic anti-leukemic effect of allogeneic hematopoietic cell transplantation (HCT) is dependent on genetic disparity between donor and recipient, intimately associated with graft-versus-host disease (GVHD), and mediated by lymphocytes contained in or derived from the donor hematopoietic cell graft. Three decades of intense effort have not identified clinical strategies that can reliably separate the graft-versus-leukemia (GVL) effect from the alloimmune reaction that drives clinical GVHD. For patients who require HCT and for whom two or more human leukocyte antigen (HLA)-A, -B, -C, and -DRB1-matched donor candidates can be identified, consideration of donor and recipient genotype at additional genetic loci both within and outside the major histocompatibility complex may offer the possibility of selecting the donor [candidate(s)] that poses the lowest probability of GVHD and the highest probability of a potent GVL effect. Strategies for engineering conventional donor lymphocyte infusion also hold promise for prevention or improved treatment of post-transplant relapse. The brightest prospects for selectively enhancing the anti-leukemic efficacy of allogeneic HCT, however, are likely to be interventions that are designed to enhance specific antitumor immunity via vaccination or adoptive cell transfer, rather than those that attempt to exploit donor alloreactivity against the host. Adoptive transfer of donor-derived T cells genetically modified for tumor-specific reactivity, in particular, has the potential to transform the practice of allogeneic HCT by selectively enhancing antitumor immunity without causing GVHD.
© 2013 John Wiley & Sons A/S.
Conflict of interest statement
The authors have declared no conflicting interests.
Figures
Similar articles
-
Strategies for Enhancing and Preserving Anti-leukemia Effects Without Aggravating Graft-Versus-Host Disease.Front Immunol. 2018 Dec 21;9:3041. doi: 10.3389/fimmu.2018.03041. eCollection 2018. Front Immunol. 2018. PMID: 30619371 Free PMC article. Review.
-
HA-1H T-Cell Receptor Gene Transfer to Redirect Virus-Specific T Cells for Treatment of Hematological Malignancies After Allogeneic Stem Cell Transplantation: A Phase 1 Clinical Study.Front Immunol. 2020 Aug 20;11:1804. doi: 10.3389/fimmu.2020.01804. eCollection 2020. Front Immunol. 2020. PMID: 32973756 Free PMC article. Clinical Trial.
-
Post-hematopoietic cell transplantation control of graft-versus-host disease by donor CD425 T cells to allow an effective graft-versus-leukemia response.Biol Blood Marrow Transplant. 2003 Apr;9(4):243-56. doi: 10.1053/bbmt.2003.50027. Biol Blood Marrow Transplant. 2003. PMID: 12720217
-
Hematopoietic stem cell transplantation and cellular therapy.HLA. 2017 May;89(5):267-277. doi: 10.1111/tan.13005. HLA. 2017. PMID: 28371460 Review.
-
Antileukemia and antitumor effects of the graft-versus-host disease: a new immunovirological approach.Acta Microbiol Immunol Hung. 2010 Dec;57(4):253-347. doi: 10.1556/AMicr.57.2010.4.2. Acta Microbiol Immunol Hung. 2010. PMID: 21183421 Review.
Cited by
-
Anticancer peptides as novel immunomodulatory therapeutic candidates for cancer treatment.Explor Target Antitumor Ther. 2024;5(5):1074-1099. doi: 10.37349/etat.2024.00264. Epub 2024 Aug 21. Explor Target Antitumor Ther. 2024. PMID: 39351437 Free PMC article. Review.
-
Effect of graft-versus-host disease on outcomes after pediatric single cord blood transplantation.Bone Marrow Transplant. 2020 Jul;55(7):1430-1437. doi: 10.1038/s41409-020-0853-1. Epub 2020 Mar 11. Bone Marrow Transplant. 2020. PMID: 32161321
-
HLA-DPB1 mismatch induces a graft-versus-leukemia effect without severe acute GVHD after single-unit umbilical cord blood transplantation.Leukemia. 2018 Jan;32(1):168-175. doi: 10.1038/leu.2017.202. Epub 2017 Jun 27. Leukemia. 2018. PMID: 28652579
-
Donor-derived CD19-targeted T cells cause regression of malignancy persisting after allogeneic hematopoietic stem cell transplantation.Blood. 2013 Dec 12;122(25):4129-39. doi: 10.1182/blood-2013-08-519413. Epub 2013 Sep 20. Blood. 2013. PMID: 24055823 Free PMC article. Clinical Trial.
-
Therapeutic Vaccines for Hematological Cancers: A Scoping Review of This Immunotherapeutic Approach as Alternative to the Treatment of These Malignancies.Vaccines (Basel). 2025 Jan 23;13(2):114. doi: 10.3390/vaccines13020114. Vaccines (Basel). 2025. PMID: 40006660 Free PMC article. Review.
References
-
- Weiden PL, Flournoy N, Thomas ED, et al. Antileukemic effect of graft-versus-host disease in human recipients of allogeneic-marrow grafts. N Engl J Med. 1979;300:1068–73. - PubMed
-
- Weiden PL, Sullivan KM, Flournoy N, Storb R, Thomas ED. Antileukemic effect of chronic graft-versus-host disease: contribution to improved survival after allogeneic marrow transplantation. N Engl J Med. 1981;304:1529–33. - PubMed
-
- Horowitz MM, Gale RP, Sondel PM, et al. Graft-versus-leukemia reactions after bone marrow transplantation. Blood. 1990;75:555–62. - PubMed
-
- Gratwohl A, Brand R, Apperley J, et al. Graft-versus-host disease and outcome in HLA-identical sibling transplantations for chronic myeloid leukemia. Blood. 2002;100:3877–86. - PubMed
-
- Stern M, de Wreede LC, Brand R, et al. Impact of graft-versus-host disease on relapse after allogeneic hematopoietic stem cell transplantation, an EBMT megafile study. ASH Annual Meeting Abstracts. 2012;120:469.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
