

Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis
- PMID: 23511840
- PMCID: PMC3694995
- DOI: 10.1097/SLA.0b013e3182895bb0
Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis
Abstract
Objective: To perform a systematic review and meta-analysis of studies comparing operative to nonoperative therapy in adult FC patients. Outcomes were duration of mechanical ventilation (DMV), intensive care unit length of stay (ICULOS), hospital length of stay (HLOS), mortality, incidence of pneumonia, and tracheostomy.
Background: Flail chest (FC) results in paradoxical chest wall movement, altered respiratory mechanics, and frequent respiratory failure. Despite advances in ventilatory management, FC remains associated with significant morbidity and mortality. Operative fixation of the flail segment has been advocated as an adjunct to supportive care, but no definitive clinical trial exists to delineate the role of surgery.
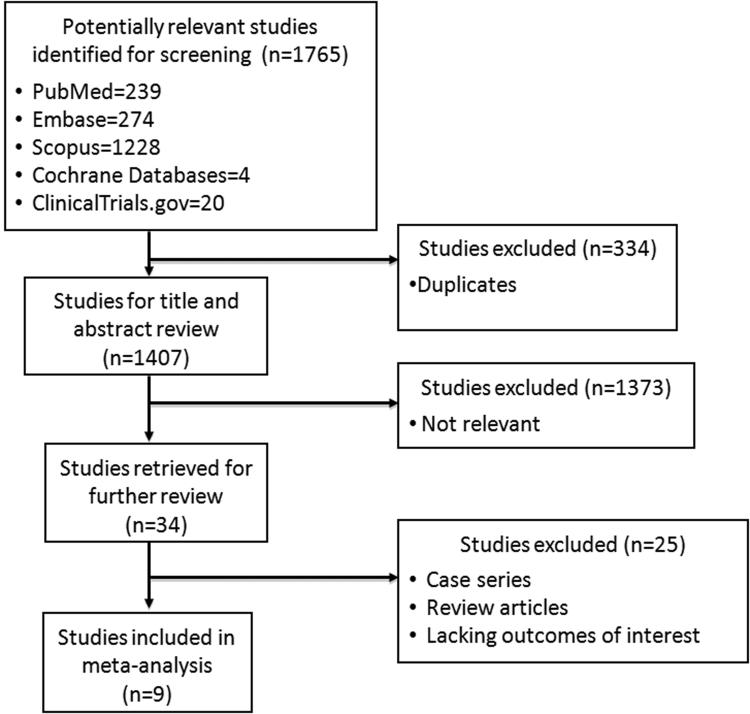
Methods: A comprehensive search of 5 electronic databases was performed to identify randomized controlled trials and observational studies (cohort or case-control). Pooled effect size (ES) or relative risk (RR) was calculated using a fixed or random effects model, as appropriate.
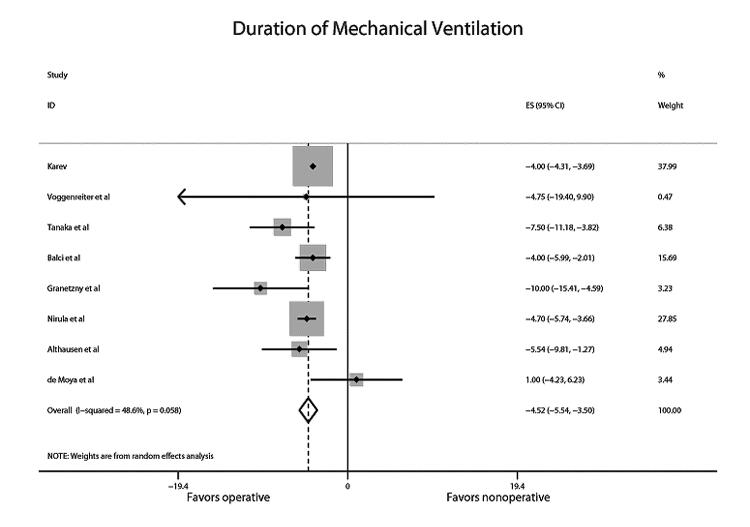
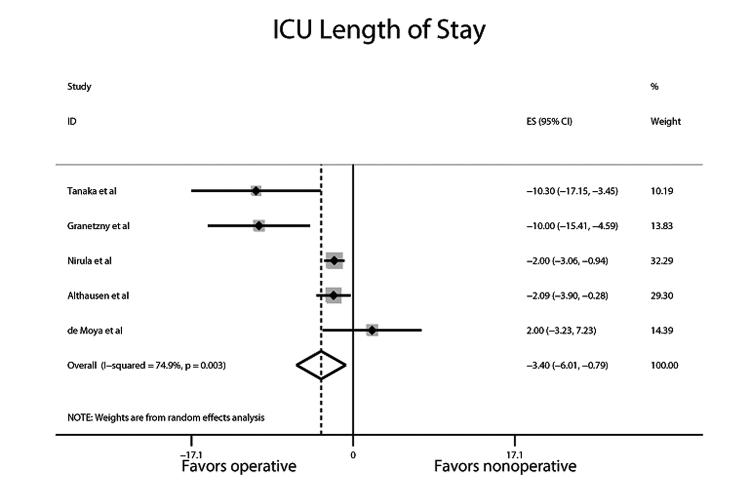
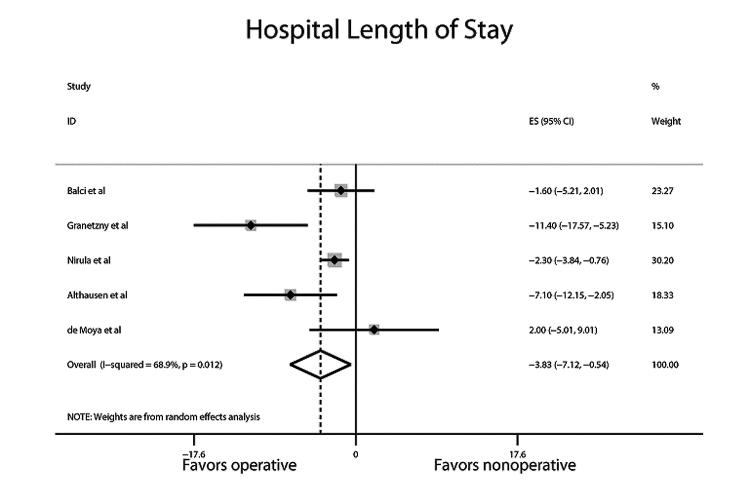
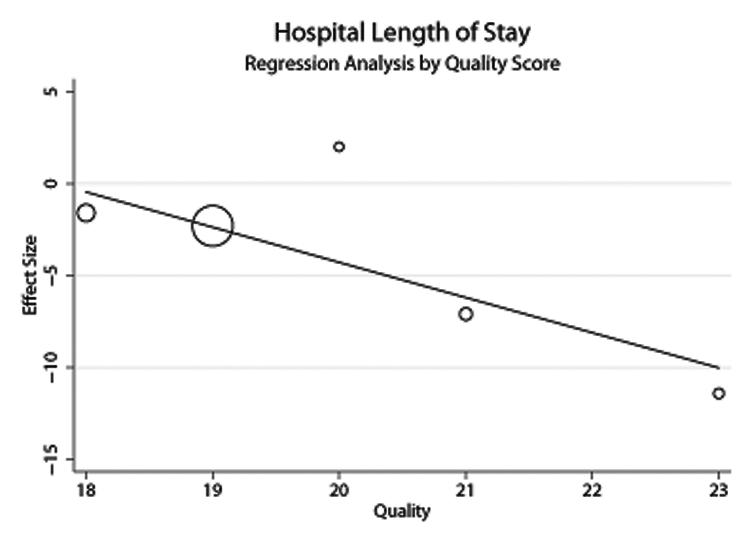
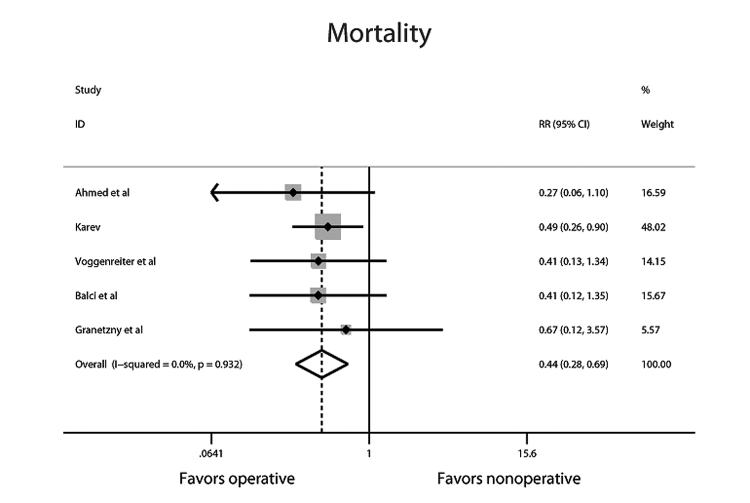
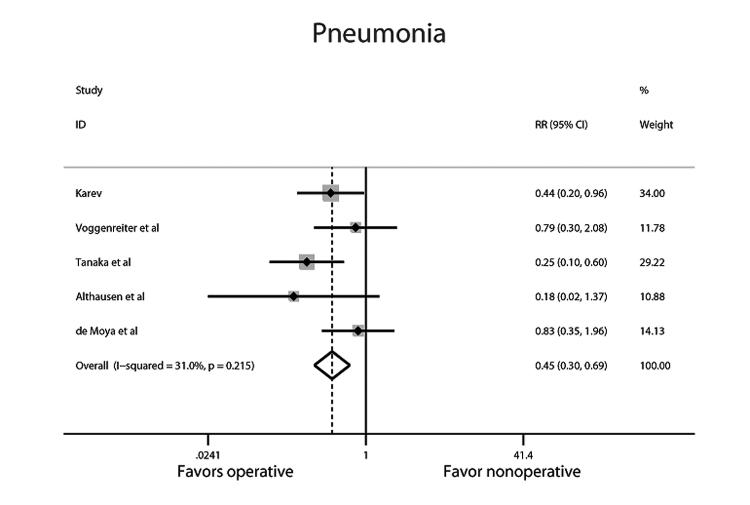
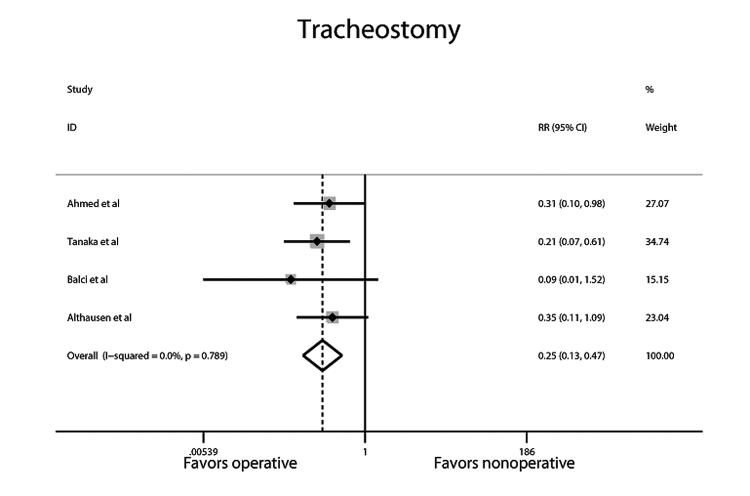
Results: Nine studies with a total of 538 patients met inclusion criteria. Compared with control treatment, operative management of FC was associated with shorter DMV [pooled ES: -4.52 days; 95% confidence interval (CI): -5.54 to -3.50], ICULOS (-3.40 days; 95% CI: -6.01 to -0.79), HLOS (-3.82 days; 95% CI: -7.12 to -0.54), and decreased mortality (pooled RR: 0.44; 95% CI: 0.28-0.69), pneumonia (0.45; 95% CI: 0.30-0.69), and tracheostomy (0.25; 95% CI: 0.13-0.47).
Conclusions: As compared with nonoperative therapy, operative fixation of FC is associated with reductions in DMV, LOS, mortality, and complications associated with prolonged MV. These findings support the need for an adequately powered clinical study to further define the role of this intervention.
Figures
References
-
- Simon B, Ebert J, Bokhari F, et al. [6/12/12];Practice Management Guideline for Pulmonary Contusion-Flail Chest. EAST Practice Management Workgroup for Pulmonary Contusion-Flail Chest. 2006 Jun; Accessed online www.east.org.
-
- Champion HR, Copes WS, Sacco WJ, et al. The Major Trauma Outcome Study: establishing national norms for trauma care. J Trauma. 1990 Nov;30(11):1356–65. - PubMed
-
- Lafferty PM, Anavian J, Will RE, et al. Operative Treatment of Chest Wall Injuries: Indications, Technique, and Outcomes. J Bone Joint Surg Am. 2011;93(1):97–110. - PubMed
-
- Ahmed Z, Mohyuddin Z. Management of Flail chest injury: internal fixation vs endotracheal intubation and ventilation. J Thorac Cardiovasc Surg. 1995;110:1676–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
