

Training practitioners to deliver opportunistic multiple behaviour change counselling in primary care: a cluster randomised trial
- PMID: 23512758
- PMCID: PMC3601942
- DOI: 10.1136/bmj.f1191
Training practitioners to deliver opportunistic multiple behaviour change counselling in primary care: a cluster randomised trial
Abstract
Objectives: To evaluate the effect of training primary care health professionals in behaviour change counselling on the proportion of patients self reporting change in four risk behaviours (smoking, alcohol use, exercise, and healthy eating).
Design: Cluster randomised trial with general practices as the unit of randomisation.
Setting: General practices in Wales.
Participants: 53 general practitioners and practice nurses from 27 general practices (one each at all but one practice) recruited 1827 patients who screened positive for at least one risky behaviour.
Intervention: Behaviour change counselling was developed from motivational interviewing to enable clinicians to enhance patients' motivation to change health related behaviour. Clinicians were trained using a blended learning programme called Talking Lifestyles.
Main outcome measures: Proportion of patients who reported making beneficial changes in at least one of the four risky behaviours at three months.
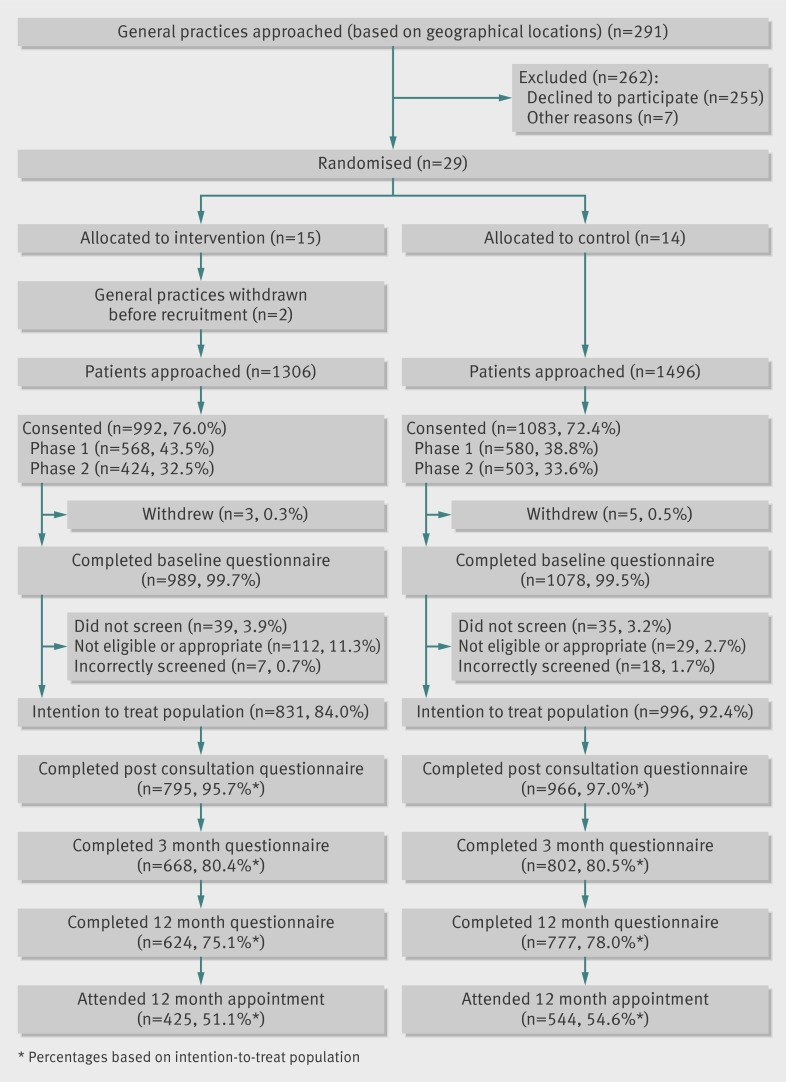
Results: 1308 patients from 13 intervention and 1496 from 14 control practices were approached: 76% and 72% respectively agreed to participate, with 831 (84%) and 996 (92%) respectively screening eligible for an intervention. There was no effect on the primary outcome (beneficial change in behaviour) at three months (362 (44%) v 404 (41%), odds ratio 1.12 (95% CI 0.90 to 1.39)) or on biochemical or biometric measures at 12 months. More patients who had consulted with trained clinicians recalled consultation discussion about a health behaviour (724/795 (91%) v 531/966 (55%), odds ratio 12.44 (5.85 to 26.46)) and intended to change (599/831 (72%) v 491/996 (49%), odds ratio 2.88 (2.05 to 4.05)). More intervention practice patients reported making an attempt to change (328 (39%) v 317 (32%), odds ratio 1.40 (1.15 to 1.70)), a sustained behaviour change at three months (288 (35%) v 280 (28%), odds ratio 1.36 (1.11 to 1.65)), and reported slightly greater improvements in healthy eating at three and 12 months, plus improved activity at 12 months. Training cost £1597 per practice.
Discussion: Training primary care clinicians in behaviour change counselling using a brief blended learning programme did not increase patients reported beneficial behaviour change at three months or improve biometric and a biochemical measure at 12 months, but it did increase patients' recollection of discussing behaviour change with their clinicians, intentions to change, attempts to change, and perceptions of having made a lasting change at three months. Enduring behaviour change and improvements in biometric measures are unlikely after a single routine consultation with a clinician trained in behaviour change counselling without additional intervention.
Trial registration: ISRCTN 22495456.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Training practitioners in primary care to deliver lifestyle advice.BMJ. 2013 Mar 19;346:f1763. doi: 10.1136/bmj.f1763. BMJ. 2013. PMID: 23512762 No abstract available.
References
-
- Healthy Ambitions. Delivering Healthy Ambitions: better for less. Making every contact count. www.healthyambitions.co.uk/Uploads/BetterForLess/08%20BETTER%20FOR%20LES....
-
- Wanless D. Securing good health for the whole population: final report. HM Treasusury, 2004.
-
- Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fortmann SP, et al. AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 Update: Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. American Heart Association Science Advisory and Coordinating Committee. Circulation 2002;106:388-91. - PubMed
-
- Scarborough P, Bhatnagar P, Wickramasinghe KK, Allender S, Foster C, Rayner M.. The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: an update to 2006-07 NHS costs. J Public Health Res (Oxf) 2011;33:527-35. - PubMed
-
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA 2004;291:1238-45. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources