

Impact of primary molecular cytogenetic abnormalities and risk of progression in smoldering multiple myeloma
- PMID: 23515097
- PMCID: PMC3773463
- DOI: 10.1038/leu.2013.86
Impact of primary molecular cytogenetic abnormalities and risk of progression in smoldering multiple myeloma
Abstract
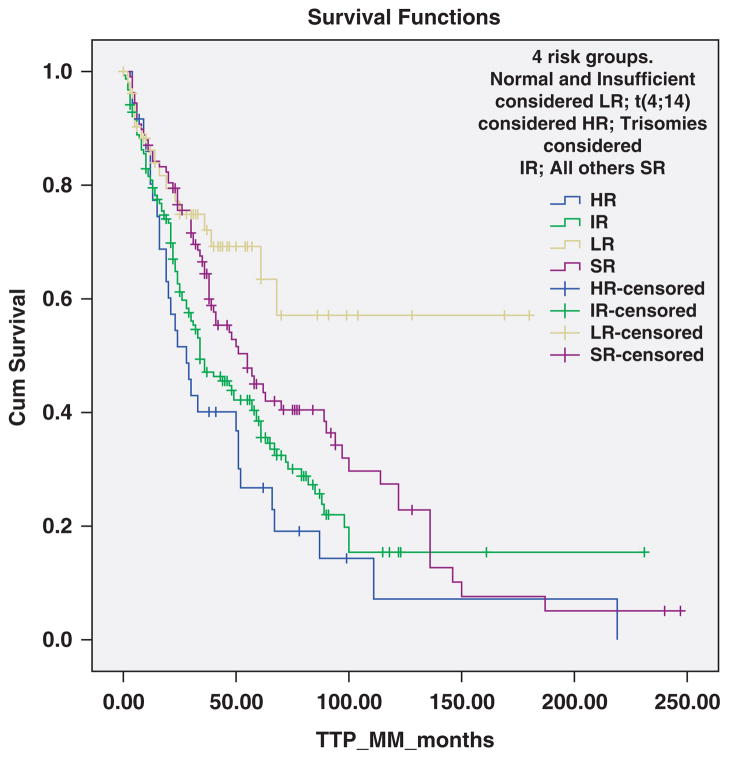
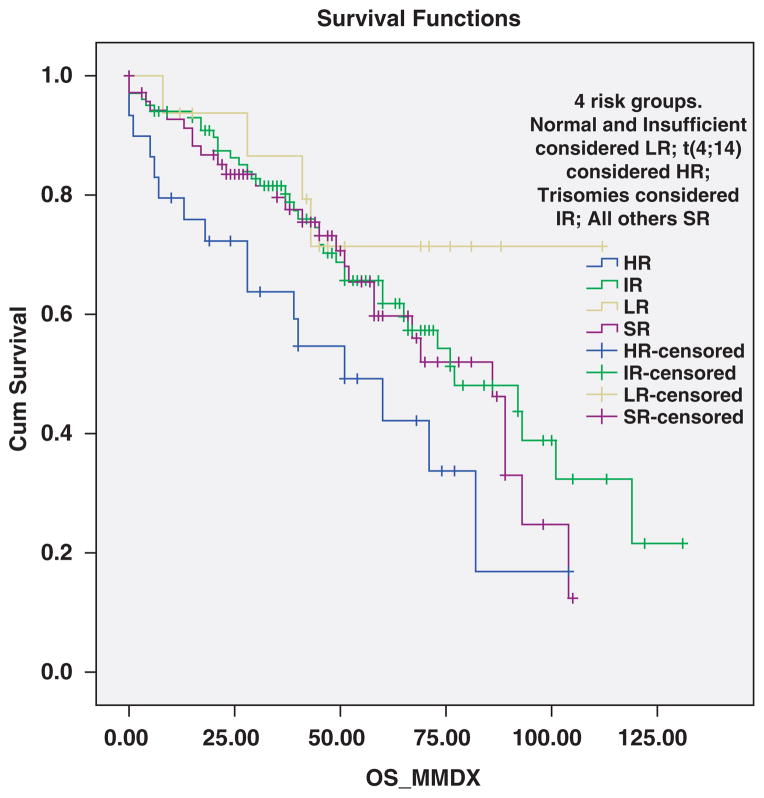
We studied 351 patients with smoldering multiple myeloma (SMM) in whom the underlying primary molecular cytogenetic subtype could be determined based on cytoplasmic immunoglobulin fluorescent in situ hybridization studies. Hundred and fifty-four patients (43.9%) had trisomies, 127 (36.2%) had immunoglobulin heavy chain (IgH) translocations, 14 (4%) both trisomies and IgH translocations, 53 (15.1%) no abnormalities detected and 3 (0.9%) had monosomy13/del(13q) in the absence of any other abnormality. Among 127 patients with IgH translocations, 57 were t(11;14), 36 t(4;14), 11 musculoaponeurotic fibrosarcoma (MAF) translocations, and 23 other or unknown IgH translocation partner. Time to progression (TTP) to symptomatic multiple myeloma was significantly shorter in patients with the t(4;14) compared with patients with t(11;14), median 28 versus 55 months, respectively, P=0.025. The median TTP was 28 months with t(4;14) (high-risk), 34 months with trisomies alone (intermediate-risk), 55 months with t(11;14), MAF translocations, other/unknown IgH translocations, monosomy13/del(13q) without other abnormalities, and those with both trisomies and IgH translocations (standard-risk), and not reached in patients with no detectable abnormalities (low-risk), P=0.001. There was a trend to shorter TTP with deletion 17p (median TTP, 24 months). Overall survival from diagnosis of SMM was significantly inferior with t(4;14) compared with t(11;14), median 105 versus 147 months, respectively, P=0.036.
Conflict of interest statement
Dr Fonseca has received a patent for the prognostication of MM based on genetic categorization of the disease. He has received consulting fees from Medtronic, Otsuka, Celgene, Genzyme, BMS, Lilly, Onyx, Binding Site, Millenium and AMGEN. He also has sponsored research from Cylene and Onyx. The remaining authors declare no conflict of interest.
Figures



References
-
- Rajkumar SV. Multiple myeloma: 2013 update on diagnosis, risk-stratification, and management. Am J Hematol. 2013;88:225–235. - PubMed
-
- Sinha S, Lacy M, Mikhael J, Hayman S, Buadi F, Detweiler-Short K, et al. Response to salvage therapies and outcome in patients with multiple myeloma relapsing after pomalidomide therapy. Leukemia. 2012;26:839–841. - PubMed
-
- Mohty B, El-Cheikh J, Yakoub-Agha I, Avet-Loiseau H, Moreau P, Mohty M. Treatment strategies in relapsed and refractory multiple myeloma: a focus on drug sequencing and ‘retreatment’ approaches in the era of novel agents. Leukemia. 2012;26:73–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
