

A phase I trial of vorinostat and alvocidib in patients with relapsed, refractory, or poor prognosis acute leukemia, or refractory anemia with excess blasts-2
- PMID: 23515411
- PMCID: PMC3618599
- DOI: 10.1158/1078-0432.CCR-12-2926
A phase I trial of vorinostat and alvocidib in patients with relapsed, refractory, or poor prognosis acute leukemia, or refractory anemia with excess blasts-2
Abstract
Purpose: This phase I study was conducted to identify the maximum-tolerated dose (MTD) of alvocidib when combined with vorinostat in patients with relapsed, refractory, or poor prognosis acute leukemia, or refractory anemia with excess blasts-2. Secondary objectives included investigating the pharmacokinetic and pharmacodynamic effects of the combination.
Experimental design: Patients received vorinostat (200 mg orally, three times a day, for 14 days) on a 21-day cycle, combined with 2 different alvocidib administration schedules: a 1-hour intravenous infusion, daily × 5; or a 30-minute loading infusion followed by a 4-hour maintenance infusion, weekly × 2. The alvocidib dose was escalated using a standard 3+3 design.
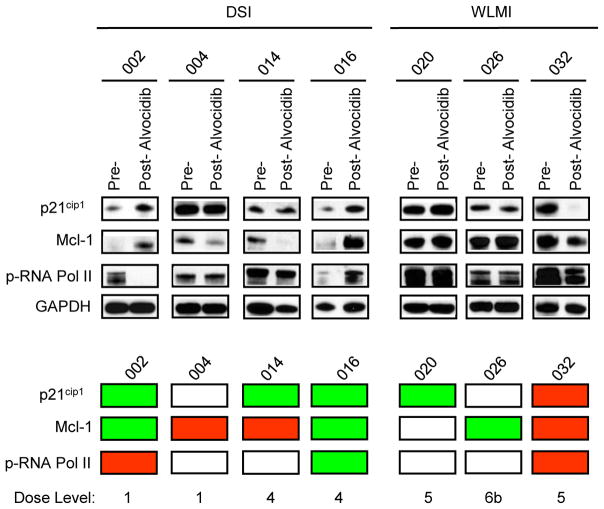
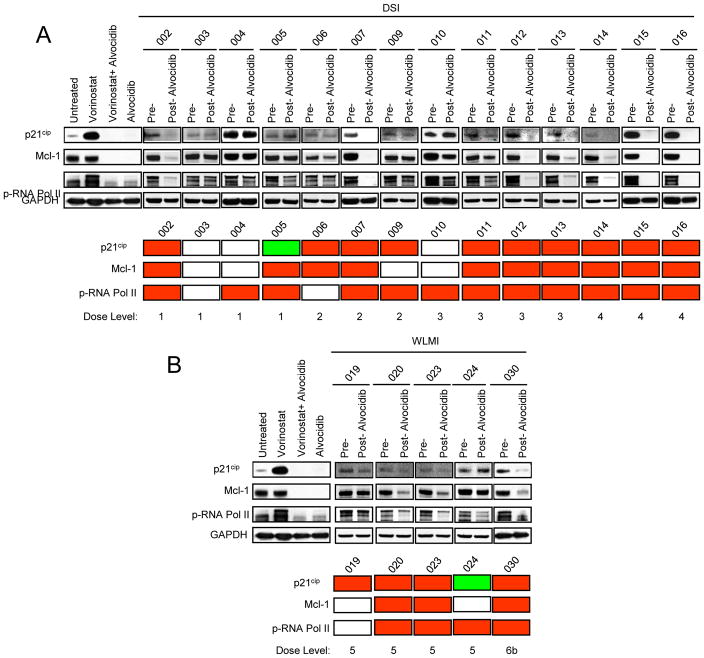
Results: Twenty-eight patients were enrolled and treated. The alvocidib MTD was 20 mg/m(2) (30-minute loading infusion) followed by 20 mg/m(2) (4-hour maintenance infusion) on days one and eight, in combination with vorinostat. The most frequently encountered toxicities were cytopenias, fatigue, hyperglycemia, hypokalemia, hypophosphatemia, and QT prolongation. Dose-limiting toxicities (DLT) were cardiac arrhythmia-atrial fibrillation and QT prolongation. No objective responses were achieved although 13 of 26 evaluable patients exhibited stable disease. Alvocidib seemed to alter vorinostat pharmacokinetics, whereas alvocidib pharmacokinetics were unaffected by vorinostat. Ex vivo exposure of leukemia cells to plasma obtained from patients after alvocidib treatment blocked vorinostat-mediated p21(CIP1) induction and downregulated Mcl-1 and p-RNA Pol II for some specimens, although parallel in vivo bone marrow responses were infrequent.
Conclusions: Alvocidib combined with vorinostat is well tolerated. Although disease stabilization occurred in some heavily pretreated patients, objective responses were not obtained with these schedules.
©2013 AACR.
Conflict of interest statement
Figures
References
-
- Roboz GJ, Giles FJ, List AF, Cortes JE, Carlin R, Kowalski M, et al. Phase 1 study of PTK787/ZK 222584, a small molecule tyrosine kinase receptor inhibitor, for the treatment of acute myeloid leukemia and myelodysplastic syndrome. Leukemia. 2006;20:952–7. - PubMed
-
- Marks P, Rifkind RA, Richon VM, Breslow R, Miller T, Kelly WK. Histone deacetylases and cancer: causes and therapies. Nat Rev Cancer. 2001;1:194–202. - PubMed
-
- Bolden JE, Peart MJ, Johnstone RW. Anticancer activities of histone deacetylase inhibitors. Nat Rev Drug Discov. 2006;5:769–84. - PubMed
-
- Olsen EA, Kim YH, Kuzel TM, Pacheco TR, Foss FM, Parker S, et al. Phase IIb multicenter trial of vorinostat in patients with persistent, progressive, or treatment refractory cutaneous T-cell lymphoma. J Clin Oncol. 2007;25:3109–15. - PubMed
-
- Garcia-Manero G, Yang H, Bueso-Ramos C, Ferrajoli A, Cortes J, Wierda WG, et al. Phase 1 study of the histone deacetylase inhibitor vorinostat (suberoylanilide hydroxamic acid [SAHA]) in patients with advanced leukemias and myelodysplastic syndromes. Blood. 2008;111:1060–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
