

Post-treatment HIV-1 controllers with a long-term virological remission after the interruption of early initiated antiretroviral therapy ANRS VISCONTI Study
- PMID: 23516360
- PMCID: PMC3597518
- DOI: 10.1371/journal.ppat.1003211
Post-treatment HIV-1 controllers with a long-term virological remission after the interruption of early initiated antiretroviral therapy ANRS VISCONTI Study
Abstract
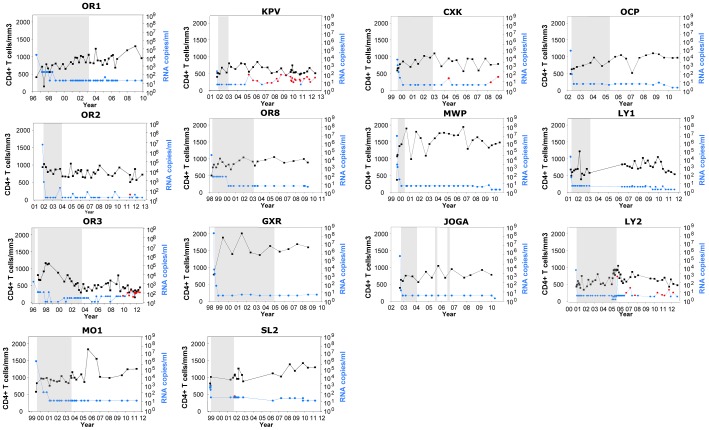
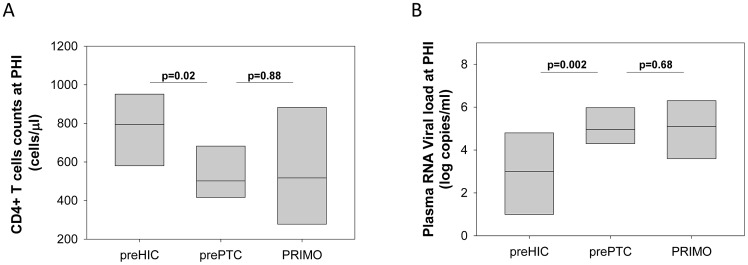
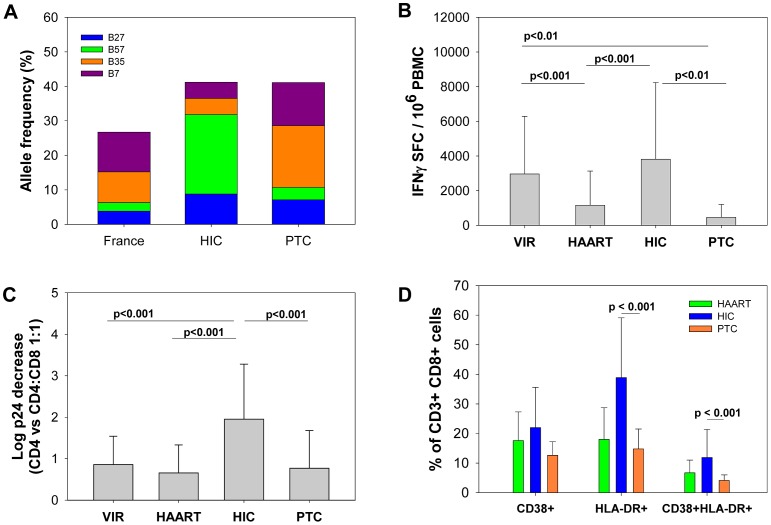
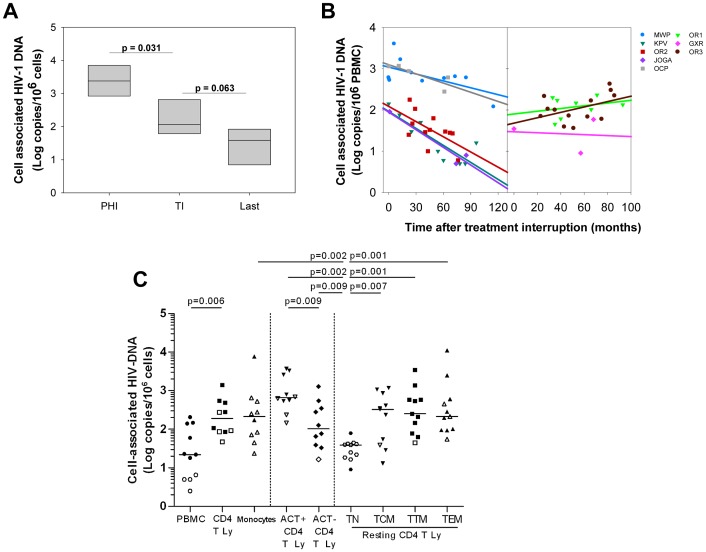
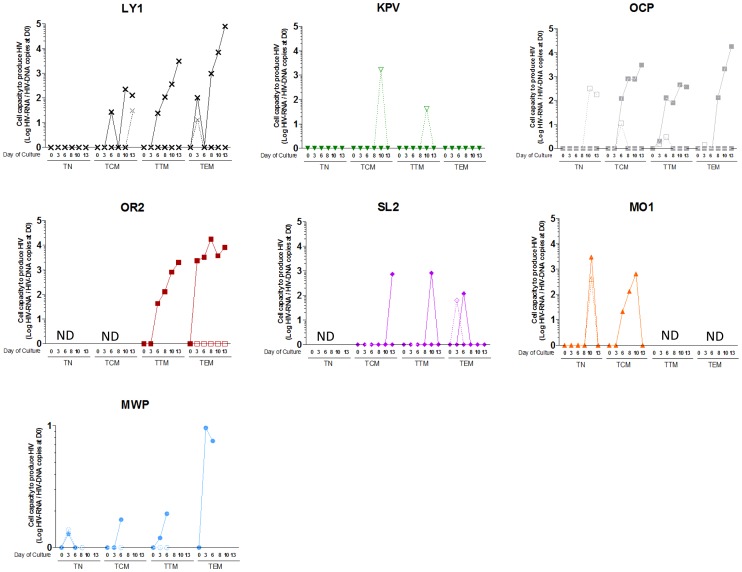
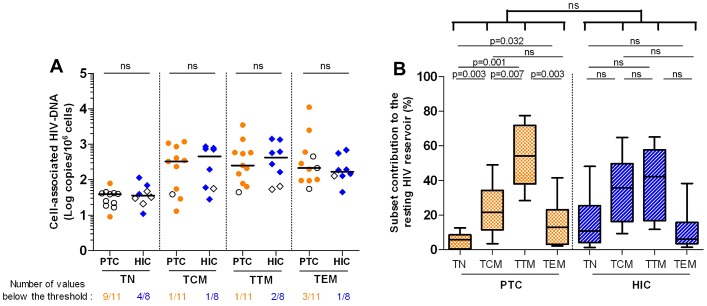
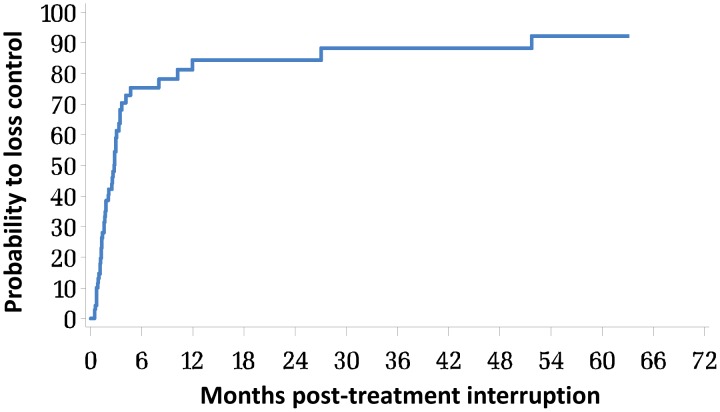
Combination antiretroviral therapy (cART) reduces HIV-associated morbidities and mortalities but cannot cure the infection. Given the difficulty of eradicating HIV-1, a functional cure for HIV-infected patients appears to be a more reachable short-term goal. We identified 14 HIV patients (post-treatment controllers [PTCs]) whose viremia remained controlled for several years after the interruption of prolonged cART initiated during the primary infection. Most PTCs lacked the protective HLA B alleles that are overrepresented in spontaneous HIV controllers (HICs); instead, they carried risk-associated HLA alleles that were largely absent among the HICs. Accordingly, the PTCs had poorer CD8+ T cell responses and more severe primary infections than the HICs did. Moreover, the incidence of viral control after the interruption of early antiretroviral therapy was higher among the PTCs than has been reported for spontaneous control. Off therapy, the PTCs were able to maintain and, in some cases, further reduce an extremely low viral reservoir. We found that long-lived HIV-infected CD4+ T cells contributed poorly to the total resting HIV reservoir in the PTCs because of a low rate of infection of naïve T cells and a skewed distribution of resting memory CD4+ T cell subsets. Our results show that early and prolonged cART may allow some individuals with a rather unfavorable background to achieve long-term infection control and may have important implications in the search for a functional HIV cure.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Wong JK, Hezareh M, Gunthard HF, Havlir DV, Ignacio CC, et al. (1997) Recovery of replication-competent HIV despite prolonged suppression of plasma viremia. Science 278: 1291–1295. - PubMed
-
- Bongiovanni M, Casana M, Tincati C, d'Arminio Monforte A (2006) Treatment interruptions in HIV-infected subjects. J Antimicrob Chemother 58: 502–505. - PubMed
-
- Yerly S, Kaiser L, Perneger TV, Cone RW, Opravil M, et al. (2000) Time of initiation of antiretroviral therapy: impact on HIV-1 viraemia. The Swiss HIV Cohort Study. AIDS 14: 243–249. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
