

Loss of Siglec-14 reduces the risk of chronic obstructive pulmonary disease exacerbation
- PMID: 23519826
- PMCID: PMC3718857
- DOI: 10.1007/s00018-013-1311-7
Loss of Siglec-14 reduces the risk of chronic obstructive pulmonary disease exacerbation
Abstract
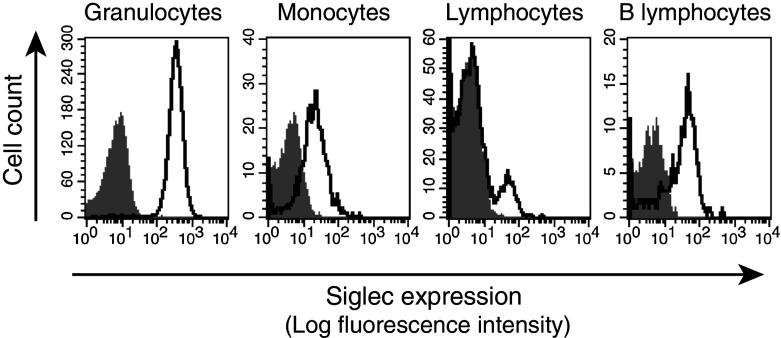
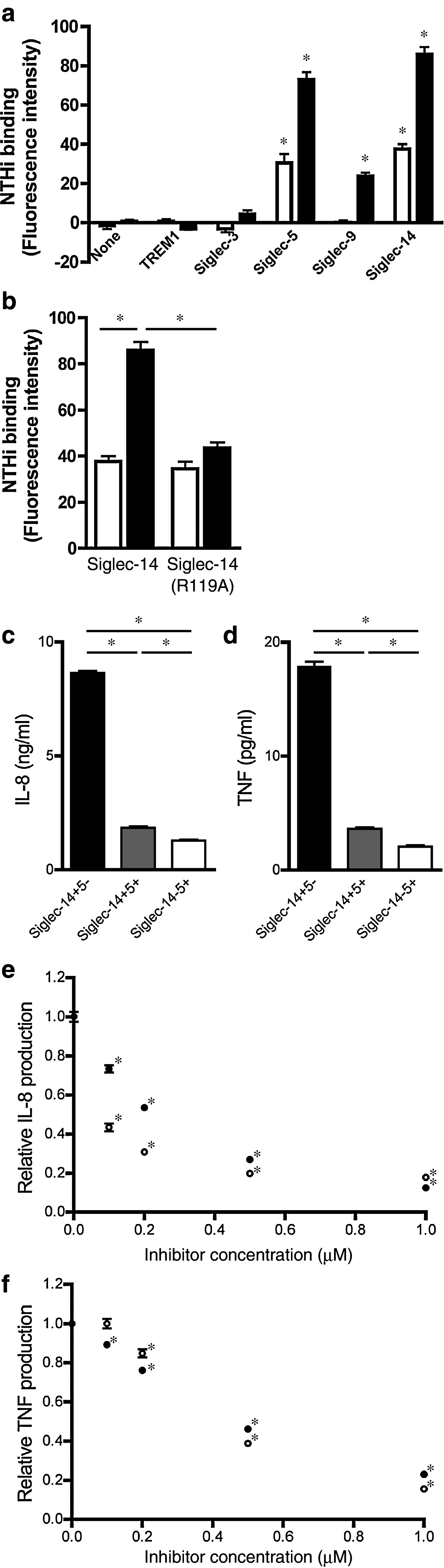
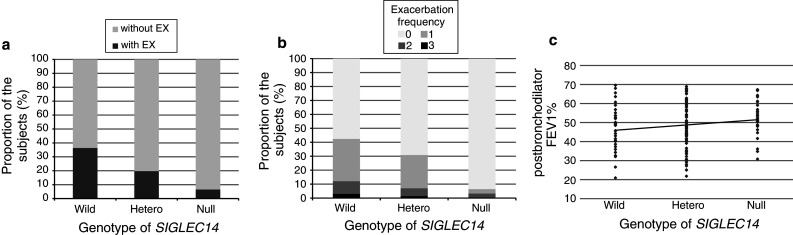
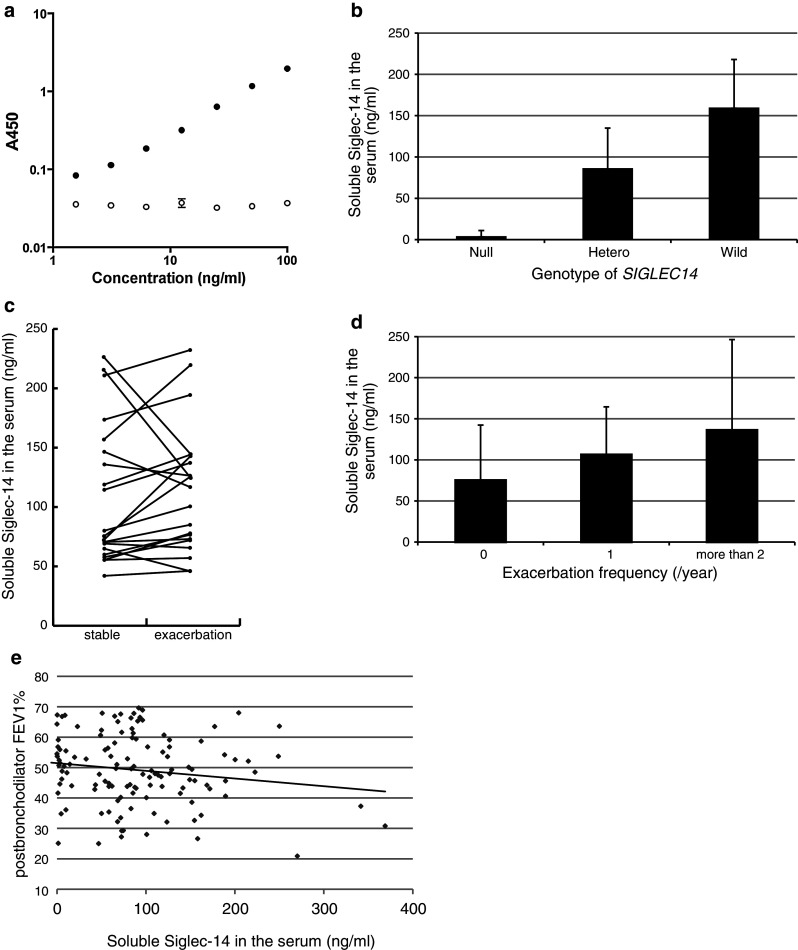
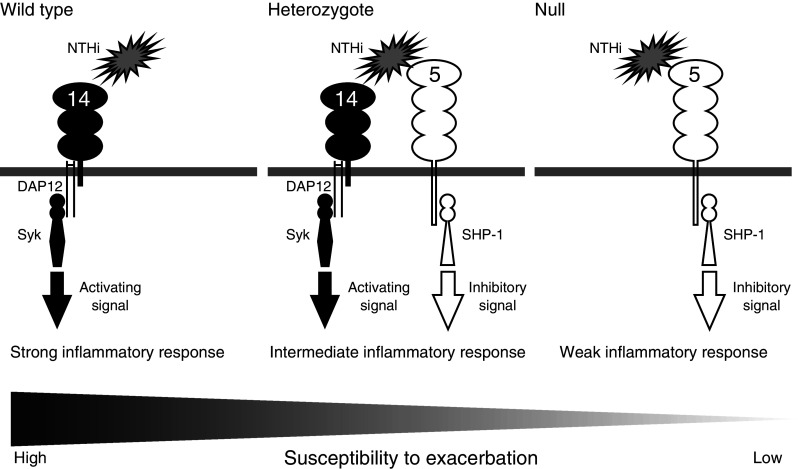
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality worldwide. COPD exacerbation, or episodic worsening of symptoms, often results in hospitalization and increased mortality rates. Airway infections by new bacterial strains, such as nontypeable Haemophilus influenzae (NTHi), are a major cause of COPD exacerbation. NTHi express lipooligosaccharides that contain sialic acids, and may interact with Siglec-14, a sialic acid recognition protein on myeloid cells that serves as an activating signal transduction receptor. A null allele polymorphism in SIGLEC14 may attenuate the inflammatory responses to NTHi by eliminating Siglec-14 expression. We asked if the loss of Siglec-14 attenuates the inflammatory response by myeloid cells against NTHi, and if the SIGLEC14-null polymorphism has any effect on COPD exacerbation. We found that NTHi interacts with Siglec-14 to enhance proinflammatory cytokine production in a tissue culture model. Inhibitors of the Syk tyrosine kinase suppress this response. Loss of Siglec-14, due to SIGLEC14-null allele homozygosity, is associated with a reduced risk of COPD exacerbation in a Japanese patient population. Taken together, Siglec-14 and its downstream signaling pathway facilitate the "infection-inflammation-exacerbation" axis of COPD disease progression, and may represent promising targets for therapeutic intervention.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- World Health Organization . World Health Statistics 2008. Geneva: WHO; 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
