

Outcomes in UK patients with hospital-acquired bacteraemia and the risk of catheter-associated urinary tract infections
- PMID: 23520064
- PMCID: PMC3664375
- DOI: 10.1136/postgradmedj-2012-131393
Outcomes in UK patients with hospital-acquired bacteraemia and the risk of catheter-associated urinary tract infections
Abstract
Purpose: There is lack of contemporary outcome data on patients with hospital-acquired infections that cause bacteraemia. We determined the risk factors for 7-day mortality and investigated the hypothesis that, compared with central venous catheter (CVC)-associated bacteraemic infections, catheter-associated bacteraemic urinary tract infections (UTIs) were significantly associated with 7-day mortality.
Methods: From October 2007 to September 2008, demographical, clinical and microbiological data were collected on patients with hospital-acquired bacteraemia. Patients were followed until death, hospital discharge or recovery from infection. Risk factors for 7-day mortality were determined and multivariate logistic regression was used to define the association between catheter-associated bacteraemic UTIs and likelihood of death.
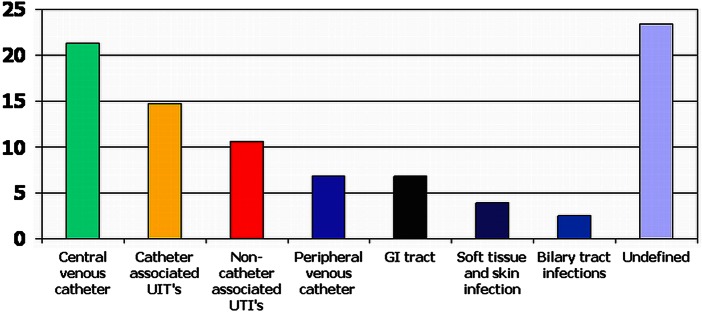
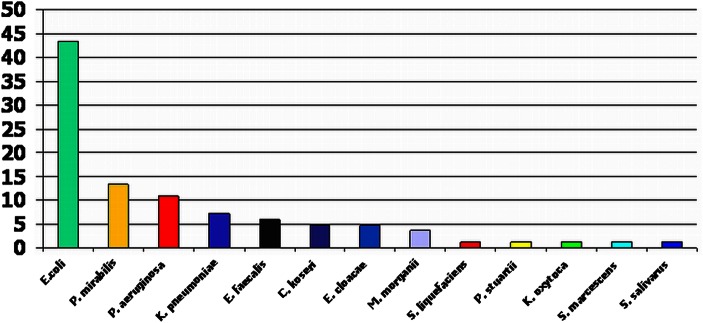
Results: 559 bacteraemic episodes occurred in 437 patients. Overall, there were 90 deaths (20.6%) at 7 days and 153 deaths (35.0%) at 30 days. Among patients with catheter-associated bacteraemic UTIs, 7-day and 30-day mortalities associated with each bacteraemic episode were 25/83 (30.1%) and 33/83 (39.8%), respectively. Within this subgroup, the commonest isolates were Escherichia coli, 36 (43.4%), Proteus mirabilis, 11 (13.3%) and Pseudomonas aeruginosa, 9 (10.8%). There were 22 (26.5%) multiple drug-resistant isolates and, of the E coli infections, 6 (16.7%) were extended spectrum β-lactamase producers. In univariate analysis, the variables found to have the strongest association with 7-day mortality were age, Pitt score, Charlson comorbidity index (CCI), medical speciality and site of infection. Compared with CVC-associated bacteraemic infections, there was a significant association between catheter-associated bacteraemic UTIs and 7-day mortality (OR 4.16, 95% CI 1.86 to 9.33). After adjustment for age and CCI, this association remained significant (OR 2.90, 95% CI 1.19 to 7.07).
Conclusions: Compared with CVC-associated bacteraemic infections, catheter-associated bacteraemic UTIs were significantly associated with 7-day mortality. Efforts to reduce these infections should be prioritised.
Keywords: Bacteraemia; Catheter associated UTI; Hospital-acquired.
Figures
References
-
- National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control 2004;32:470–85 - PubMed
-
- Coello R, Charlett A, Ward V, et al. Device related sources of bacteraemia in English hospitals. Opportunities for the prevention of hospital-acquired bacteraemia. J Hosp Infect 2003;53:46–57 - PubMed
-
- Jain P, Parada JP, David A, et al. Overuse of the indwelling urinary tract catheter in hospitalised medical patients. Arch Inter Med 1995;155:1425–29 - PubMed
-
- Gardam MA, Amihod B, Orenstein P, et al. Overutilization of indwelling urinary catheters and the development of nosocomial urinary tract infections. Clin Perform Qual Health Care 1998;6:99–102 - PubMed
-
- Wald HL, Epstein AM, Radcliff TA, et al. Extended use of urinary catheters in older surgical patients: a patient safety problem? Infect Control Hosp Epidemiol 2008;29:116–24 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
