

Review
doi: 10.2337/dc12-1805.
Type 2 diabetes: etiology and reversibility
Affiliations
- PMID: 23520370
- PMCID: PMC3609491
- DOI: 10.2337/dc12-1805
Item in Clipboard
Review
Type 2 diabetes: etiology and reversibility
Diabetes Care.
2013 Apr.
No abstract available
Figures

A: Fasting plasma glucose and weight change 2 years after randomization either to gastric banding or to intensive medical therapy for weight loss and glucose control. Data plotted with permission from Dixon et al. (13). B: Early changes in fasting plasma glucose level following pancreatoduodenal bypass surgery. A decrease into the normal range was seen within 7 days. Reproduced with permission from Taylor (98).

Effect of a very-low-calorie diet in type 2 diabetes on fasting plasma glucose level (A), basal hepatic glucose production (HGP) (B), and hepatic triacylglycerol content (C). For comparison, data for a matched nondiabetic control group are shown as ○. Reproduced with permission from Lim et al. (21). FFM, fat-free mass.
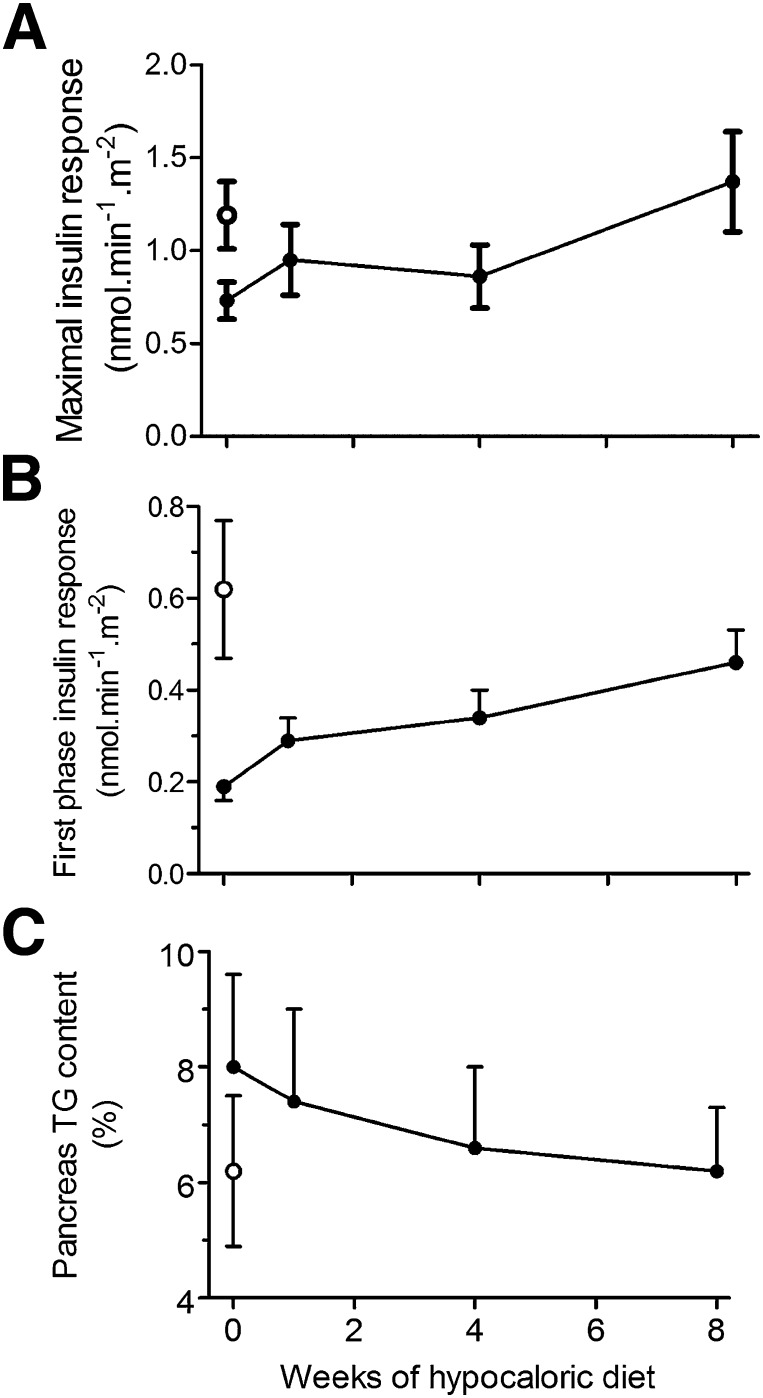
Effect of an 8-week very-low-calorie diet in type 2 diabetes on arginine-induced maximal insulin secretion (A), first phase insulin response to a 2.8 mmol/L increase in plasma glucose (B), and pancreas triacylglycerol (TG) content (C). For comparison, data for a matched nondiabetic control group are shown as ○. Replotted with permission from Lim et al. (21).

Mechanism of interaction between excess amounts of fatty acids, diacylglycerol, and ceramide and insulin action within the hepatocyte. Diacylglycerol activates PKCε and inhibits activation of IRS-1 by the insulin receptor. Ceramides cause sequestration of Akt2 by PKCζ and inhibit insulin control of gluconeogenesis. These mechanisms have recently been reviewed (99). FFA, free-fatty acid; TG, triacylglycerol.

Change in fasting plasma glucose (A), 2 h post-oral glucose tolerance test (B), and homeostasis model assessment (HOMA-B) insulin secretion (C) during the 16-year follow-up in the Whitehall II study. Of the 6,538 people studied, diabetes developed in 505. Time 0 was taken as the diagnosis of diabetes or as the end of follow-up for those remaining normoglycemic. Redrawn with permission from Tabák et al. (80).

The twin cycle hypothesis of the etiology of type 2 diabetes. During long-term intake of more calories than are expended each day, any excess carbohydrate must undergo de novo lipogenesis, which particularly promotes fat accumulation in the liver. Because insulin stimulates de novo lipogenesis, individuals with a degree of insulin resistance (determined by family or lifestyle factors) will accumulate liver fat more readily than others because of higher plasma insulin levels. In turn, the increased liver fat will cause relative resistance to insulin suppression of hepatic glucose production. Over many years, a modest increase in fasting plasma glucose level will stimulate increased basal insulin secretion rates to maintain euglycemia. The consequent hyperinsulinemia will further increase the conversion of excess calories to liver fat. A cycle of hyperinsulinemia and blunted suppression of hepatic glucose production becomes established. Fatty liver leads to increased export of VLDL triacylglycerol (85), which will increase fat delivery to all tissues, including the islets. This process is further stimulated by elevated plasma glucose levels (85). Excess fatty acid availability in the pancreatic islet would be expected to impair the acute insulin secretion in response to ingested food, and at a certain level of fatty acid exposure, postprandial hyperglycemia will supervene. The hyperglycemia will further increase insulin secretion rates, with consequent enhancement of hepatic lipogenesis, spinning the liver cycle faster and driving the pancreas cycle. Eventually, the fatty acid and glucose inhibitory effects on the islets reach a trigger level that leads to a relatively sudden onset of clinical diabetes. Figure adapted with permission from Taylor (98).
References
-
- Turner RC, Cull CA, Frighi V, Holman RR, UK Prospective Diabetes Study (UKPDS) Group Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). JAMA 1999;281:2005–2012 - PubMed
-
- Ferrannini E, Nannipieri M, Williams K, Gonzales C, Haffner SM, Stern MP. Mode of onset of type 2 diabetes from normal or impaired glucose tolerance. Diabetes 2004;53:160–165 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
