

Impact of waist circumference and body mass index on risk of cardiometabolic disorder and cardiovascular disease in Chinese adults: a national diabetes and metabolic disorders survey
- PMID: 23520466
- PMCID: PMC3592870
- DOI: 10.1371/journal.pone.0057319
Impact of waist circumference and body mass index on risk of cardiometabolic disorder and cardiovascular disease in Chinese adults: a national diabetes and metabolic disorders survey
Abstract
Background: We updated the prevalence of obesity and evaluated the clinical utility of separate and combined waist circumference (WC) or body mass index (BMI) category increments in identifying cardiometabolic disorder (CMD) and cardiovascular disease (CVD) risk in Chinese adults.
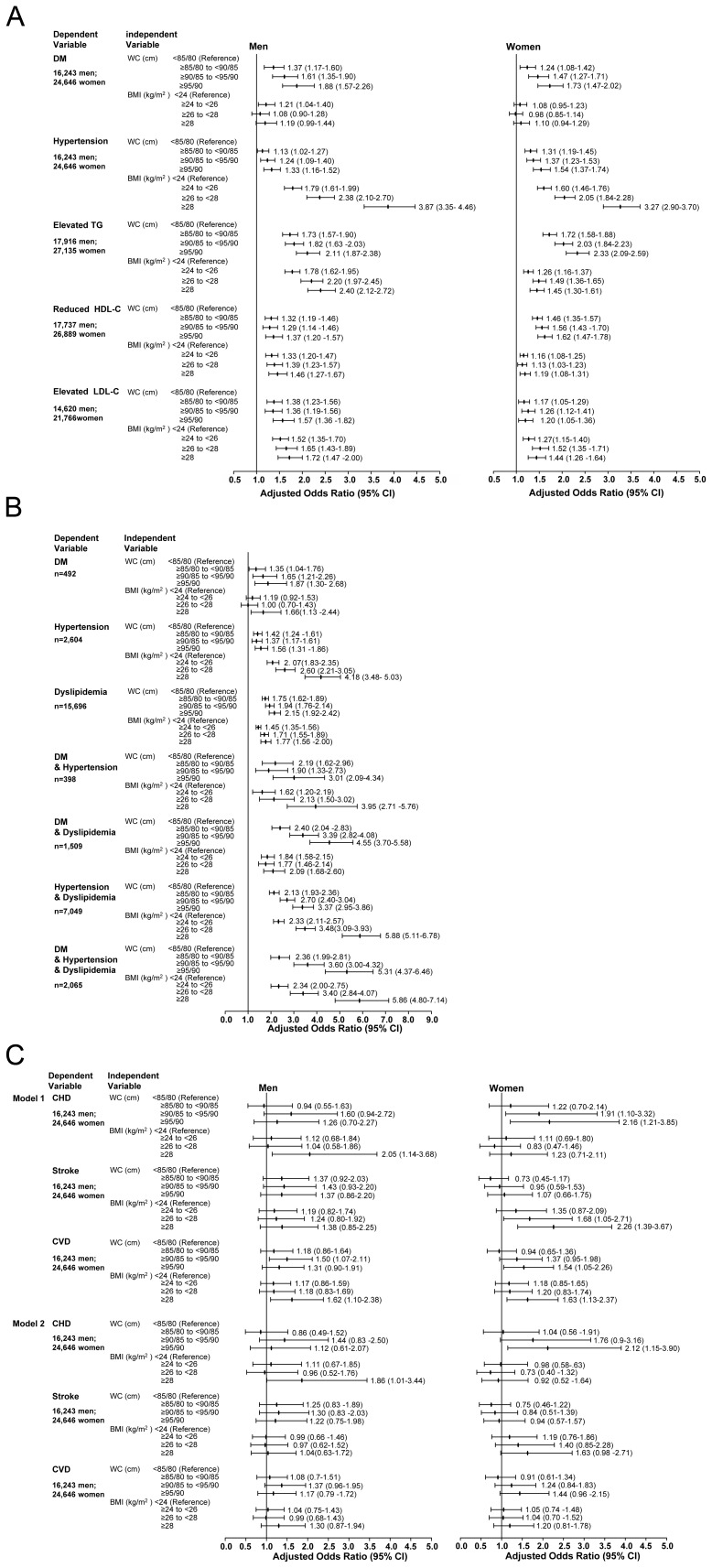
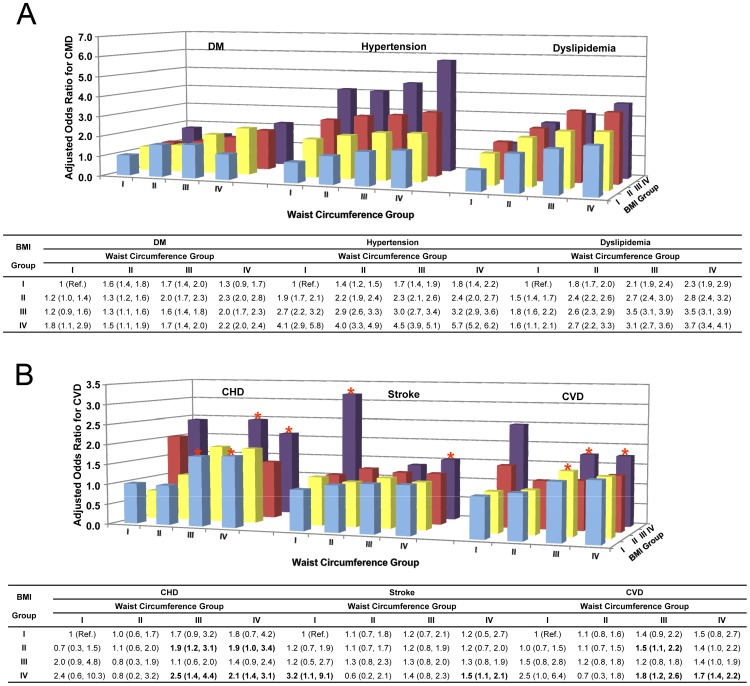
Methods and findings: 46,024 participants aged ≥20 years, a nationally representative sample surveyed in 2007-2008, were included in this analysis. Taking the cutoffs recommended by the Chinese Joint Committee for Developing Chinese Guidelines (JCDCG) and the Working Group on Obesity in China (WGOC) into account, the participants were divided into four WC and four BMI groups in 0.5-SD increments around the mean, and 16 cross-tabulated combination groups of WC and BMI. 27.1%, 31.4%, and 12.2% of Chinese adults are centrally obese, overweight, or obese according to JCDCG and WGOC criteria. After adjustment for confounders, after a 1-SD increment, WC is associated with a 1.7-fold or 2.2-fold greater risk of having DM or DM plus dyslipidemia than BMI, while BMI was associated with a 2.3-fold or 1.7-fold higher hypertension or hypertension plus dyslipidemia risk than WC. The combination of WC and BMI categories had stronger association with CMD risk, i.e., the adjusted ORs (95% CI) of having DM, hypertension, and dyslipidemia for the combined and separate highest WC and BMI categories were 2.19 (1.96-2.44) vs 1.88 (1.67-2.12) and 1.12 (0.99-1.26); 5.70 (5.24-6.19) vs 1.51 (1.39-1.65) and 1.69 (1.57-1.82); and 3.73 (3.42-4.07) vs 2.16 (1.98-2.35) and 1.33 (1.25-1.40), respectively. The combination of WC and BMI categories was more likely to identify individuals with lower WC and lower BMI at CVD risk, even after the effects of CMD were controlled (all P<0.05).
Conclusion: Central obesity, overweight, and obesity are epidemic in Chinese adults. The combination of WC and BMI measures is superior to the separate indices in identifying CMD and CVD risk.
Conflict of interest statement
Figures
References
-
- Smith SC Jr (2010) Screening for high-risk cardiovascular disease: a challenge for the guidelines: comment on “systematic review of guidelines on cardiovascular risk assessment: which recommendations should clinicians follow for a cardiovascular health check?”. Arch Intern Med 170: 40–42. - PubMed
-
- Yang ZJ, Liu J, Ge JP, Chen L, Zhao ZG, et al. (2012) Prevalence of cardiovascular disease risk factor in the Chinese population: the 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur Heart J 33: 213–220. - PubMed
-
- Van Gaal LF, Mertens IL, De Block CE (2006) Mechanisms linking obesity with cardiovascular disease. Nature 444: 875–880. - PubMed
-
- Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, et al. (2002) Obesity and the risk of heart failure. N Engl J Med 347: 305–313. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
